Article
Johana Enyd Cifuentes Rodríguez 1
Sandra Guerrero Gamboa 2
* This work is derived from the doctoral research proyect named: "M.A.T.E.O. viabilidad y efecto de una intervención de automanejo para pacientes con úlceras venosas".
* Artículo derivado del proyecto de investigación doctoral titulado: "M.A.T.E.O. viabilidad y efecto de una intervención de automanejo para pacientes con úlceras venosas".
* Artigo derivado do projeto de pesquisa de doutorado chamado "M.A.T.E.O. viabilidad y efecto de una intervención de automanejo para pacientes con úlceras venosas".
1 ![]() 0000-0001-5384-3480. Universidad Nacional de Colombia, Colombia. jecifuentesr@unal.edu.co
0000-0001-5384-3480. Universidad Nacional de Colombia, Colombia. jecifuentesr@unal.edu.co
2 ![]() 0000-0002-0893-0478. Universidad Nacional de Colombia, Colombia. nsguerrerog@unal.edu.co
0000-0002-0893-0478. Universidad Nacional de Colombia, Colombia. nsguerrerog@unal.edu.co
Received: 10/08/2019
Sent to peers: 12/09/2019
Approved by peers: 11/12/2019
Accepted: 18/12/2019
Para citar este artículo / To reference this article / Para citar este artigo: Cifuentes JE, Guerrero S. Nursing Interventions Aimed at Persons with Venous Ulcers: an Integrative Review. Aquichan. 2020;20(1):e2017. DOI: https://doi.org/10.5294/aqui.2020.20.1.7
Theme: Evidence-based practice.
Contribution to the discipline: Identifying the elements that shaped nursing interventions in other cultures and the foundations underlying them, permits knowing progress in the area, as well as strengths and weaknesses in their development and execution. In turn, testing nursing interventions in keeping with our context, that is, those addressing human beings with their needs, doubts, and fears – through viable learning and mutual construction settings favor positive care experiences. Providing quality and cost-effective care requires viable, effective, easily replicable nursing interventions with important social impact, which transform the nursing practice and demonstrate their autonomy and jurisdiction.
|
Abstract Objectives: This
work sought to identify and describe the theoretical foundations, components,
duration, delivery mode, and results of the nursing interventions aimed at
persons with venous ulcers as available in the literature. Keywords (Source DeCS): Varicose ulcer; leg ulcer; nursing care; controlled before-after studies; practical nursing. |
Resumen Objetivos: identificar y describir los fundamentos teóricos, los
componentes, la duración, el modo de entrega y los resultados de las
intervenciones de enfermería dirigidas a personas con úlceras venosas
disponibles en la literatura. Palabras clave (Fuente DeCS): Úlcera varicosa; úlcera de la pierna; atención de enfermería; estudios controlados antes y después; enfermería práctica. |
Resumo Objetivos: identificar e descrever os fundamentos teóricos, os
componentes, a duração, o modo de entrega e os resultados das intervenções de
Enfermagem dirigidas a pessoas com úlceras varicosas disponíveis na literatura. Palavras-chave (Fonte DeCS): Úlcera varicosa; úlcera da perna; cuidados de enfermagem; estudos controlados antes e depois; enfermagem prática. |
Introduction
Venous ulcers (VU), also known as varicose ulcers, are open cutaneous lesions that, generally, occur on the medial side of the lower leg, between the ankle and knee, as a result of chronic venous insufficiency and ambulatory venous hypertension. Its healing can take between four and six weeks, after their initial onset (1).
Between 75 % and 80 % of all lower limb ulcers is of venous etiology, their prevalence ranges between 0.5 % and 2.7 %, and increase with age (2, 3). It has been estimated that active VU have a mean age of 210 days, with periods of < 1 to > 67 years and up to 70 % recurrence rate within three months after wound closure (4-6). These aspects turn them into a complex chronic condition, not only for patients and their families, but also to health systems.
The role the nursing discipline has played in caring for these patients has been fundamental to now understand the complexity of living with VU in lower limbs and its negative impact in all the dimensions of the quality of life of the people. The common problems confronted by patients with VU include pain, exudate, odor, limitations in mobility, depression, anxiety, social isolation, sense of sadness, and sleep disorders (7-9). Venous ulcers, like any other chronic condition, demand long-term nursing care, significant changes in lifestyle, and adherence to therapeutic regimes by the patients. These call for using compression therapy for life (the gold standard for caring and managing VU) and prevention and maintenance strategies to avoid recurrence, like leg elevation, weight control, physical activity, skin care, and protection against lesions, among others (10, 11).
Due to the aforementioned, recently, nurses have begun to design interventions to investigate if such could contribute in healing, diminished recurrence, or improved quality of life of patients with VU, besides other physical and psychosocial variables. Identifying in the literature nursing interventions available for patients with VU permits knowing the elements that compose them and how these produce beneficial results. Hence, the objective of this review is to identify and describe the theoretical foundations, components, duration, delivery mode, and results of nursing interventions aimed at persons with VU as available in the literature.
Materials and Methods
Integrative literature review based on the method proposed by Whittemore and Knafl (12), which includes the following stages:
1. Definition of the purpose of the review: identify and describe the theoretical foundations, components, duration, delivery mode, and results of nursing interventions aimed at persons with VU as available in the literature.
2. Literature search:
a search was conducted of articles in the Pubmed, Ovidnursing, and EBSCOhost electronic databases, between 2000 and 2018, given the limited research in the
area prior to this time frame. The keywords were venous leg ulcer or varicose ulcer, nursing, interventions,
and wound healing in
English, Portuguese, and Spanish. Combinations were made with the Boolean
operators (AND, OR). The search took place between 01 January and 31 April
2018, and was updated in February 2019.
The inclusion criteria were: 1)
articles published in indexed journals; 2) descriptive, experimental, and
quasi-experimental studies developed exclusively by nursing; and 3) articles
clearly presenting the development or implementation of the intervention. The
work included reviews, Masters and PhD theses, unpublished articles, as well as
studies centered on diagnostic methods or intervention studies with laboratory
products or pharmaceutical companies.
3. Data assessment: during this stage, seeking to estimate their methodological quality, the critical reading was made of the articles selected, under criteria proposed by the Joanna Briggs Institute (13). Consequently, the reviewers examined the titles independently, in function of the abstract, excluding irrelevant studies; thereafter, they selected the articles according to the inclusion criteria and examined each of the articles independently.
4. Data analysis: a work instrument was designed to extract the principal characteristics of the studies included in the analysis. The instrument was composed of the following sections: 1) identification data of the study, author, year, and country; 2) study objective; 3) study design and sample; 4) description of the intervention: type of intervention, theoretical foundation, components, duration and delivery mode; and 5) intervention result variables. For their classification according to their level of evidence, the work followed the criteria proposed by the Joanna Briggs Institute (13). The final stage of the review describes the findings through the synthesis of the information and is presented hereinafter.
Results
According to their content, 207 studies were found, of which 42 were discarded due to duplication in the databases; then, the titles and abstracts of the remaining articles were revised, according to the inclusion and exclusion criteria; finally, three reviewers, through consensus, kept 16 articles in the review.
In this review, 16 articles fulfilled the search criteria and were included. Of these, 50 % (8) were carried out in countries in Oceania; 25 % (4) in Europe; 12.5 % (2) in North America; 6.25 % (1) in Asia; and 6.25 % (1) in South America (Table 1).
According with their design, the studies were: quantitative, randomized clinical trial type (10); pre and post-test with a single group (3); quasi-experimental (1); prospective with control group (1); and comparative (1). Levels of evidence prevailed in levels I and II (Table 1).
The 16 articles included 1249 patients from different community nursing care centers, outpatient injury and dermatology clinics, and care services to patients with tissue disturbance in university hospitals. Among the participants, female sex had the highest prevalence, and age ranged between 54 and 80 years.
Figure 1. Study selection process
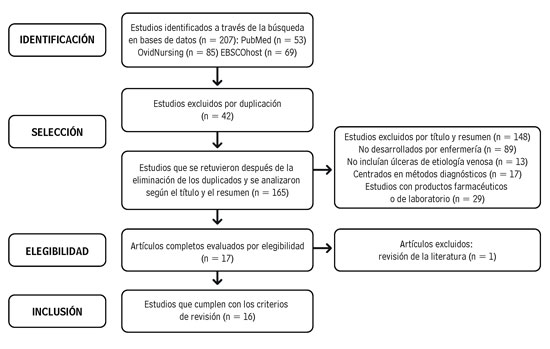
Source: Own elaboration.
Target population
Herein, 100 % of the interventions were aimed at patients with VU; their relatives or caregivers were not considered.
Type of intervention and theoretical foundation
Of the 16 interventions found in the studies, 11 were educational (14-24); among these, four promoted the development of progressive resistance exercises (14, 18, 19, 21); two, of clinical characteristics, evaluated change in the quality of life of patients receiving a system of four-layer and short stretch compression bandage; and three were community type (25, 26).
The cognitive social theory by Bandura supported four educational interventions (14, 18, 22, 24). Two studies added elements from the goal setting theory by Locke, besides using the motivational interview by Miller and Rollnick as technique to facilitate behavioral change among participants during their meetings (22, 24).
The three community interventions proposed were based on the so-called Leg Club care model, which proposes that wound care take place in an informal setting (nonclinical), owned by the community (like community halls), which promote social interaction, support among peers, information exchange, health promotion, education, and continuous care for all age groups with problems related with their legs (27-29) (Table 1).
Components of the interventions
Of the interventions identified, 87.5 % (14/16) mentioned an educational component in their development (14-24, 27-29); while 12.5 % (2/16) did not conduct any type of education, given that change in VU healing rate was only observed as response to using four-layer short stretch compression systems (25, 26). Among the education themes, the review found lifestyles, causes, development, progress and prevention of VU, importance of compression bandages, adherence, self-care activities, and exercise. The last is the aspect imparted most frequently by nurses, at 62.5 % (10/16) (14-19, 21-24).
The community interventions (27-29) included assessing the health status, measuring the ankle-arm index, treating the VU, applying a short stretch compression bandage system, counseling and support regarding VU, follow up and attendance to the community’s Leg Club. All the interventions considered an essential clinical element, which was the clinical evaluation of the wound area (Table 1).
Delivery mode and duration
All the interventions took place face to face; however, 13 were delivered individually, and three collectively (27-29). Four studies had telephone follow up with the participants (14, 17, 18, 20). The first made six calls from 10 to 15 minutes to reinforce development of resistance exercises(14); the second indicated regular telephone follow up during the first, fourth, and last week, without stipulating the time (16); the third made calls only when the patient required it (18); and the fourth indicated that the two monitoring were of 30 minutes (20).
In relation with the material used to deliver the intervention, 43.7 % (7/16) of the studies was supported by booklets and brochures (14, 15, 17, 18, 20, 21, 24); while 31.5 % (5/16) did not describe this aspect (19, 22, 27, 28). The minimum time for the interventions was of eight weeks, and the maximum lasted 72 (18 months). Nevertheless, 50 % (8/16) of the interventions lasted 12 weeks (14, 16-19, 28, 29). With respect to the follow up, only one study did not monitor the participants (23); the rest showed diversity regarding its time and purpose, which ranged between weekly, biweekly, and monthly. On the time dedicated to each session with the patient, it varied from 20 to 60 minutes for the first session; the rest lasted between 10 and 30 minutes (14, 17, 20-23). Of all the interventions, 62.2 % (10/16) were delivered in clinical contexts; 18.7 % (3/16) in the patients’ homes; and 18.7 % (3/16) in the community’s Leg Club (Table 1).
Table 1. Description of the nursing interventions aimed at persons with venous ulcers
Author, year, country |
Level of evidence |
Study design and sample |
Description of the intervention: type of intervention, theoretical foundation, components, duration, delivery mode |
Variables of the result |
1. O’Brien et al., 2012, Australia (18). |
I |
RCT n = 11patients CG: 5 patients. IG: 6 patients. |
-
Educational intervention, program of progressive resistance exercises at
home. |
- The Pressure Ulcer Scale for Healing. |
2. Edwards H et al., 2005, Australia (29). |
I |
RCT n = 56 patients CG: 28 IG: 28 |
- Intervention: community. |
- Level of pain according to the Medical Outcomes
Study Pain Measures. |
3. Finlayson K et al., 2012, Australia (25). |
I |
RCT n = 87 patients Four-layer compression system group: 45 Class 3 compression stocking system group (30-35 mmHg): 42 |
-
Intervention: clinical. |
- The Pressure Ulcer Scale for Healing. |
4. Edwards H et al., 2005, Australia (28). |
I |
RCT n = 33 patients CG: 17 IG: 16 |
- Intervention: community. - Theory: Leg Club care model. - Components: equal. Edwards et al. (1). - Duration: 12 weeks. - Delivery mode: in group, weekly. - Material: not mentioned. - Place: Leg Club. - Follow up: at the start of the study and 12 weeks later. |
- Wound area: tracing of the wound and point-to-point measurement. - The Pressure Ulcer Scale for Healing. - Wound healing rate. |
5. Jull A et al., 2009, New Zealand (19). |
I |
RCT n = 39 patients CG: 19 IG: 20 |
- Intervention: educational, in relation with exercises to be done progressively. - Theory: not mentioned. - Components: not described. - Duration: 12 weeks. - Delivery mode: individually, exercises were prescribed progressively, according to assessment by the nurse. - Material: not mentioned. - Place: Care service of patients with leg ulcers. - Follow up: at the beginning and after, on weeks 3, 6, and 9. |
- Changes in calf muscle function. - Area of the ulcer (measured with the Silhouette Mobile device, ARANZ). - Healing of the ulcer. - Time to complete healing. - Air plethysmography to measure: venous volume, ejection volume, ejection fraction, residual fraction, fraction of residual fraction, and venous filling rate. |
6. Edwards H et al., 2009, Australia (27). |
I |
RCT n = 67 patients CG: 33 IG: 34 |
- Intervention: community. - Theory: Leg Club care model. - Components: equal. Edwards et al. (1). - Duration: 24 weeks. - Delivery mode: in group, weekly. - Material: not described. - Place: Leg Club. - Follow up: start, 12 and 24 weeks from recruitment. |
- Quality of life index by Spitzer. - Geriatric depression scale by Yesavage. - Self-esteem scale by Rosenberg. - Measurement of the level of pain by Sherbourne. - Social support scale by Sherbourne & Stewart. - Daily life activities index by Katz and Akpom. - The Medical Outcomes Study, to measure pain. |
7. O’Brien et al., 2016, Australia (14). |
I |
RCT n = 59 patients CG: 30 IG: 29 |
- Intervention: educational, of behavioral change. - Theory: self-efficacy. - Components: education on resistance exercises of lower limbs (walking); record of exercises and education on behavior changes; telephone follow up (6 calls from 10 to 15 minutes); adherence to the program. - Duration: 12 weeks. - Delivery mode: first meeting, face to face, during 20-30 minutes. Thereafter, via telephone. - Material: exercise booklet for people with venous ulcers, pedometer, record sheets of their series of exercises and repetitions. - Place: community nursing service. - Follow up: weekly (weeks 1, 2, 4, 6, 8, and 12), via telephone. |
Primary - Healing of the wound (yes/no). - Area de la ulcer, through digital planimetry device. - The Pressure Ulcer Healing Score. Secondary - Yale physical activity survey. – Functional ability: measurement of gait and equilibrium by Tinetti and the ankle range of motion. - Quality of life short form, SF8. - Adherence to exercise. |
8. Domingues et al., 2018, Brazil (17). |
I |
RCT n = 71 patients CG: 36 IG: 35 |
- Intervention: educational, on lifestyles. - Theory: not mentioned. - Components: physical exercise of lower limbs, compression therapy, guidance on lifestyles and rest. - Duration: 12 weeks. - Delivery mode: face to face, for 40 min. Thereafter, meetings every 4 weeks to reinforce initial instructions and clear doubts. - Material: information booklet. - Place: unit specialized in wound treatment. - Follow up: four meetings per month to reinforce lifestyle and solve doubts, and two telephone follow-up sessions. |
Primary - Reduction of the wound area in square centimeters. - Pressure Ulcer Scale for Healing. Secondary - Numerical scale of pain perception. - Quality of life, Freiburg Life Quality Assessment for Wounds. |
9. Brooks J et al., 2004, The United Kingdom (15). |
II |
Quasi-experimental study n = 102 patients CG: 60 IG: 42 |
- Intervention: educational. - Theory: not mentioned. - Components: causes, prevention, importance of the compression system, nutrition, exercise, pain management, skin care, early consultation in case of skin rupture and avoidance of leg trauma. - Duration: 52 weeks. - Delivery mode: face to face, during consultation. Education reinforcement every 3 months. - Material: information booklets with prevention measures, exercises, and importance of compression stockings. - Place: service. - Follow up: weekly, during 52 weeks. |
Primary - Venous ulcer recurrence rate Secondary - Time using compression stockings. - Difference in recurrence rates among patients who were completely mobile (mobile without aid) and had complete movement of the ankle and those with less movement and mobility of the ankle. |
10. Wong et al., 2012, Hong Kong (26). |
I |
RCT n = 276 patients Group 1:87 Group 2:95 Group 3 (control): 94 |
- Intervention: clinical. - Theory: not mentioned. - Components: application of the compression system. - Duration: 24 weeks. - Delivery mode: not described. - Material: four-layer short stretch compression bandages. - Place: service caring for patients with venous ulcers. - Follow up: start, 12 and 24 weeks from the recruitment. |
- Brief Pain Inventory (Chinese version). - The Frenchay Activities Index (Chinese version). - The Short Form-12-item, SF-12, Health Survey. - Quality of life questionnaire for patients with venous ulcers - Charing Cross Venous Ulcer Questionnaire. - Time to heal the wound and its area through digital planimetry. |
11. González A, 2014, The United States (20). |
II |
Design of a single group with pretest and post-test n = 30 patients |
- Intervention: educational. - Theory: not mentioned. - Components: development and progress of the disease, self-care activities to favor healing the venous ulcer and prevent its recurrence. - Duration: 9 weeks. - Delivery mode: individual, for 45 min; via telephone, for 30 min. - Material: guide and booklet with information regarding the intervention components. - Place: homes of patients with venous ulcers attending a center specialized in wound care. - Follow up: via telephone, during 30 minutes on weeks 2 and 9, from recruitment. |
- An ad-hoc check list that measured the process of the disease and self-care activities. - Healing the venous ulcer. - Wound recurrence at 9 weeks. |
12. Kelechi et al., 2014, The United States (21). |
IV |
Comparative Design n = 21 patients IG:12 CG:9 |
- Intervention: educational. - Theory: motivational interview approach. - Components: motivational interview and conditioning activities for the lower leg function. - Duration: 8 weeks. - Delivery mode: individually, each week until week 6. The motivational interview lasted 10 min. - Material: booklet. - Place: centers caring for people with wounds. - Follow up: at the start and at 8 weeks. |
- Analog visual scale of the pain and Leg Pain Questionnaire. - Depression: Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. - Strength: force dynamometer for ankle dorsiflexion and plantar flexion. - Range of motion: dorsiflexion goniometry, plantar flexion, inversion, eversion in degrees. - Questionnaire for Physical Activity and confidence and Exercise. - Function of physical activity: Timed Chair Rise Test, Timed Up and Go and Community Healthy Activities Model for Program for Seniors. |
13. Heinen M et al., 2012, The Netherlands (22). |
I |
Multi-center RCT n = 184 patients from 11 outpatient clinics. IG:92 CG:92 |
- Intervention: self-management program denominated Lively Legs. - Theory: cognitive social by Bandura. Included elements from the goal setting theory by Locke and Latham and the precaution adoption process model by Westein et al. Additionally, the work used the motivational interview approach by Miller and Rollnick as technique to discuss health behaviors. - Components: 6 sessions evaluating lifestyle, behavioral change, beliefs in health and education. Included demonstration and exercises. - Duration: 18 months. The first session lasted from 45 - 60 min. From the second to the sixth, from 20 - 30 min. - Delivery mode: the first session, at the start; the second, from 2 to 4 weeks after the first; and the sixth session, 6 months after the first session. - Material: not described. - Place: dermatology clinics. - Follow up: at the start, at 6, 12, and 18 months. |
Primary - Adherence to compression therapy. - Physical activity: Physical Activity Recall (IPAQ) by Craig. - Monitor physical activity: accelerometer. - The Seven-Day Physical Activity Recall Inventory. Secondary - Measurement of the wound through a plastic sheet with cells one square centimeter. |
14. Kapp et al., 2010, Australia (23). |
II |
Study of a single group with pretest and posttest n = 152 patients |
- Intervention: educational, through the leg ulcer prevention program. - Theory: not mentioned. - Components: 1) role of the compression bandage and compression stockings to favor healing the ulcer and avoid recurrence. 2) Treatment of venous ulcer. 3) Exercise and its impact on the calf muscle pump function, and leg elevation to manage edema. 4) Healthy eating. 5) Skin care. 6) Reinforcement of the use of compression stockings and maintenance of the healed ulcer. - Duration: each session, taking between 20 and 60 min to complete. The six sessions lasted three hours. - Delivery mode: weekly, face to face to patient, during the nursing home visit for wound care. - Material: on-line learning technology and printed educational material. - Place: at patients’ homes. - Follow up: not described. |
- Questionnaire designed for this study, comprised by knowledge, behaviors, attitudes, adoption, and adherence to recommendations. |
15.Van Hecke et al., 2011, Belgium (24). |
II |
Pretest and posttest assessment of a single group with qualitative approach n = 26 patients |
- Intervention: educational, cognitive and behavioral, denominated Adherence to Leg Ulcer Lifestyle Advice. - Theories: self-efficacy, goal setting, construct of representations of the disease by Leventhal et al., 1997, and motivational interview as technique to facilitate behavioral change. - Components: adherence to compression therapy, physical activity, and leg elevation. - Duration: 12 weeks. - Delivery mode: face to face to patient. - Material: a booklet and notebook of nursing work: patient registry. - Place: at patients’ homes. - Follow up: to collect quantitative data, at the start of the intervention, one week after ending the intervention and three months later. To collect qualitative data, one week after ending the intervention. |
- Semistructured interviews one week after ending the intervention. - Participant observation during nurses’ consultations in the homes. - Record of number of hours of compression, frequency and duration of leg exercises and leg elevation. - Level of activity by using the accelerometer. - Pain through the verbal scale. - Measure the healing rate of the wound through acetate tracing and computer assisted counting of square centimeters. |
16. Meagher H, et al., 2012. Ireland (16) |
IV |
Prospective, comparative study n = 35 patients IG: 18 CG: 17 |
- Intervention: educational. - Theory: not mentioned. - Components: promotion of physical activity, specifically walking. - Duration: 12 weeks. - Delivery mode: face to face at the start, and later via telephone, if required. - Material: monitor physical activity ActivPal. - Place: University Hospital. - Follow up: at the start, and on weeks 4 and 12. Thereafter, regular telephone contact, to answer questions and clear doubts. |
- Sociodemographic questionnaire. - Analog visual scale of pain. - Size of ulcer through digital planimetry. - Number of steps per each participant through an external monitor to measure activities and a pedometer. |
Result variables
Among the result variables evaluated with highest frequency, it was found: 1) measurement of the wound area (11/16) (14,16-19, 22, 24-26, 28); 2) assessment of the healing process with the scale denominated The Pressure Ulcer Scale for Healing, through aspects of wound area, amount of exudate, and type of tissue (6/16); 3) pain (7/16) (16, 17, 21, 24, 26-28); and 4) quality of life (5/16) (14,17,25-27). Regarding the instruments used to assess the results mentioned, only four studies reported the corresponding psychometric properties (21, 25-27).
Based on this integrative literature review, the recommendation is to strengthen the design and report of the interventions in this specific area of nursing knowledge. For this, entities exist, like the Medical Research Council, which offers guidelines for their construction, or the Template for intervention description and replication (TIDieR) checklist and guide (30), among others.
Discussion
The objective of this review was to identify and describe the theoretical foundations, components, duration, delivery mode, and results of nursing interventions aimed at persons with VU available in the literature. The findings described confirm the variety of nursing interventions seeking to improve care and potentiate care aimed at this population.
Although most of the interventions were educational, few mentioned the theory, concepts or proposals that guided their construction. The use of conceptual models and nursing theories facilitate understanding common problems in the practice from a unique perspective. This permits testing disciplinary knowledge, demonstrating positive results in the health of individuals, and acquiring autonomy and jurisdiction in the practice (31). As reported with the use of the nursing care model for patients with VU in Australia, denominated Leg Club, this model is based on the community; patients are treated collectively while operating without prior schedules, and incorporating a well leg regime, a preventive education and counseling program, once the ulcer heals. Its objective is to empower patients and turn them into participants in their treatment, through modification of behaviors that diminish the recurrence of VU (32-34). It has been recognized as a viable, replicable, and profitable model in The United Kingdom, Australia, and other European countries (35).
In terms of the components of the interventions, the promotion of physical activity and exercise was the central theme of the studies where it was prescribed and patients were motivated to walk and elevate their legs. Evidence exists that demonstrates the positive effect of exercise in improving the calf muscle pump function and its subsequent effects on healing VU, besides their use as complementary therapy to compression systems that, until now, are considered the gold standard in treating these types of chronic wounds (36-40). More than 50 % of the authors considered wound assessment an essential component and a positive effect of their interventions (14-19, 21, 22, 26-29).
The delivery mode was face to face; 15 studies conducted follow up, but only four specified that it was via telephone, and its objective was to reinforce the education taught (14, 16, 17, 20). Systematic literature reviews have validated the efficacy of telephone support in interventions developed by different health professionals and have reported positive results in patients, like quality of life and reduced rates of hospitalization and costs in health systems (41, 42). Consequently, the telephone calls could be a useful tool and more effective than other communication devices to offer care to patients with VU, considering that mobility impairment is one of the most common negative effects in this population.
The time invested in delivering the interventions is paramount in identifying cost-effective nursing practices. Notwithstanding, few mentioned the specific time invested in each session with patients and their follow ups. With regards to the support material, only one study used multimedia presentation (23). Probably, the use of digital media results problematic for elderly patients, who often lack the knowledge and skills needed to use electronic resources (43). However, eHealth literacy interventions could offer an opportunity to the elderly with VU, by permitting access to resources, like electronic health records, on-line support groups, and self-management tools that guide patients to solve habitual problems, make informed decisions, and communicate with health providers (44, 45). Likewise, involving relatives and caregivers would contribute to the identification, follow up, and timely control of complications related with the venous ulcer (46).
With respect to the result variables, two aspects are highlighted; the first has to do with the psychometric properties of the instruments used to measure the result variables proposed, given that only four studies did so, and most of the scales used were not specific for patients with VU. This could be explained by the limited number of specific instruments available for patients with VU. Concretely, six instruments have been identified for this type of population, but such have demonstrated poor criterion and construct validity. Additionally, generic questionnaires, like the EQ-5D and the SF-36 of quality of life evidenced weak response capacity, or did not support their use in patients with VU (47). These aspects would have important repercussions on the validity of the data reported. Secondly, the fact that clinical aspects prevail, like wound healing and the healing process against other variables. Empirical evidence exists that holds that wound healing processes are complex, and these affect physical, psychological, and even sociological factors, in favorable or unfavorable manner (5, 48-53). With this, it must be stated that, although the clinical-type variables as objectives are important, including behavioral variables is also important. It is likely, in many cases, to achieve significant behavioral changes, but not clinical in the short term.
In consequence, it is not possible to rule that a nursing intervention is effective if it did not manage to get patients with VU to heal their wounds in a given time, but it is possible perhaps if it contributed to improving they experience and cope with this chronic health condition. Thus, the question would be if it is pertinent to establish as results only clinical variables in this type of population.
Limitations
The articles included were published only in English, so that studies in other languages and contexts could ratify or contradict the way the interventions are developed and the results expected. The lack of specific instruments for patients with VU and the use of other generic questionnaires without satisfactory validity tests could limit the interpretation of the results. This review did not include in its search interventions aimed at caregivers or relatives of patients with VU.
Conclusions
The findings presented in this integrative review permit identifying the existence of few nursing interventions aimed at persons with VU, although it is a chronic condition that tends to increase its incidence and prevalence. Unfortunately, less than half of the studies mentioned the theoretical foundation supporting the intervention, and those which did so did not expose which concepts or propositions were selected as guides in their development. Diversity existed regarding the delivery time of the intervention and the dynamics of the face-to-face meetings, as well as the follow up carried out. Few studies reported the thematic content of their interventions, a fact that limits understanding if these generate impact or not on the primary results established, with the priority being the venous ulcer healing. It is considered necessary to rethink the approach of nursing interventions in this area of knowledge, given the prevalence of people as holistic beings, and the object of nursing is that of caring for the human health experience.
Conflict of interests: none declared.
Acknowledgements: Johana Cifuentes thanks the Academic Direction at Universidad Nacional de Colombia for the scholarship granted to conduct her PhD studies.
References
1. Harding K, Dowsett C, Fias L, Jelnes R, Mosti G, Oien R, et al. Simplifying venous leg ulcer management. 2015 [cited 2019 Mar. 20]. Available in: https://www.woundsinternational.com/resources/details/simplifying-venous-leg-ulcer-management-consensus-recommendations
2. Xie T, Ye J, Rerkasem K, Mani R. The venous ulcer continues to be a clinical challenge: An update. Burn Trauma. [Internet]. 2018;6(18):1-7. DOI: https://doi.org/10.1186/s41038-018-0119-y
3. Berenguer-Pérez M, López-Casanova P, Sarabia-Lavín R, González de la Torre H, Verdú-Soriano J. Epidemiology of venous leg ulcers in primary health care: Incidence and prevalence in a health centre: A time series study ( 2010-2014 ). Int Wound J. [Internet]. 2019;16(1):256-65. DOI: https://doi.org/10.1111/iwj.13026
4. González-Consuegra RV, Verdú J. Quality of life in people with venous leg ulcers: An integrative review. J Adv Nurs. [Internet]. 2011;67(5):926-44. DOI: https://doi.org/10.1111/j.1365-2648.2010.05568.x
5. Finlayson K, Wu M-L, Edwards HE. Identifying risk factors and protective factors for venous leg ulcer recurrence using a theoretical approach: A longitudinal study. Int J Nurs Stud. [Internet]. 2015;52(6):1042-51. DOI: https://doi.org/10.1016/j.ijnurstu.2015.02.016
6. De Araujo ICF, Yoshida WB, Abbade LPF, Deffune E. The pernicious cycle of VLUs in Brazil: Epidemiology, pathogeny and auxiliary healing methods. J Wound Care. [Internet]. 2013;22(4):186-93. DOI: https://doi.org/10.12968/jowc.2013.22.4.186
7. Hopkins A. Disrupted lives: Investigating coping strategies for non-healing leg ulcers. Br J Nurs. [Internet]. 2004;13(9):556-63. DOI: https://doi.org/10.12968/bjon.2004.13.9.12972
8. Green J, Jester R, McKinley R, Pooler A. The impact of chronic venous leg ulcers: A systematic review. J Wound Care. [Internet]. 2014;23(12):601–12. DOI: https://doi.org/10.12968/jowc.2014.23.12.601
9. Briggs M, Flemming K. Living with leg ulceration: A synthesis of qualitative research. J Adv Nurs. [Internet]. 2007;59(4):319-28. DOI: https://doi.org/10.1111/j.1365-2648.2007.04348.x
10. Marinel Lo Roura J, Verdú Soriano J. Conferencia Nacional de Consenso sobre las Úlceras de la Extremidad Inferior. 2nd ed. Madrid: Ergon; 2018. 146 p.
11. Alavi A, Sibbald RG, Phillips TJ, Miller OF, Margolis DJ, Marston W, et al. What’s new: Management of venous leg ulcers treating venous leg ulcers. J Am Acad Dermatol. [Internet]. 2016;74(4):643-64. DOI: https://doi.org/10.1016/j.jaad.2015.03.059
12. Whittemore R, Knafl K. The integrative review: Updated methodology. J Adv Nurs. [Internet]. 2005;52(5):546-53. DOI: https://doi.org/10.1111/j.1365-2648.2005.03621.x
13. The Joanna Briggs Institue. New JBI Levels of Evidence [Internet]. New JBI Levels of Evidence. 2013 [cited 2019 Feb. 21]. Available in: http://joannabriggs.org/assets/docs/approach/JBI-Levels-of-evidence_2014.pdf
14. O’Brien J, Finlayson K, Kerr G, Edwards H. Evaluating the effectiveness of a self-management exercise intervention on wound healing, functional ability and health-related quality of life outcomes in adults with venous leg ulcers: A randomised controlled trial. Int Wound J. [Internet]. 2016;14(1):1-8. DOI: https://doi.org/10.1111/iwj.12571
15. Brooks J, Ersser SJ, Lloyd A, Ryan TJ. Nurse-led education sets out to improve patient concordance and prevent recurrence of leg ulcers. J Wound Care. [Internet]. 2004;13(3):111-6. DOI: https://doi.org/10.12968/jowc.2004.13.3.26585
16. Meagher H, Ryan D, Clarke-Moloney M, O’Laighin G, Grace PA. An experimental study of prescribed walking in the management of venous leg ulcers. J Wound Care. [Internet]. 2012;21(9):421-430. DOI: https://doi.org/10.12968/jowc.2012.21.9.421
17. Domingues E, Oliveira U, Lima MHM. Effectiveness of the strategies of an orientation programme for the lifestyle and wound-healing process in patients with venous ulcer: A randomised controlled trial. Int Wound J. [Internet]. 2018;15(5):798-806. DOI: https://doi.org/10.1111/iwj.12930
18. O’Brien J, Edwards H, Stewart I, Gibbs H. A home-based progressive resistance exercise programme for patients with venous leg ulcers: A feasibility study. Int Wound J. [Internet]. 2012;10(4):389–96. DOI: https://doi.org/10.1111/j.1742-481X.2012.00995.x
19. Jull A, Parag V, Walker N, Maddison R, Kerse N, Johns T. The PREPARE pilot RCT of home-based progressive resistance exercises for venous leg ulcers. J Wound Care. [Internet]. 2009;18(2):497–503. DOI: https://doi.org/10.12968/jowc.2009.18.12.45606
20. González A. Education project to improve venous stasis self-management knowledge. J Wound Ostomy Cont Nurs. [Internet]. 2014;41(6):556-9. DOI: https://doi.org/10.1097/WON.0000000000000088
21. Kelechi TJ, Mueller M, Spencer C, Rinard B, Loftis G. The effect of a nurse-directed intervention to reduce pain and improve behavioral and physical outcomes in patients with critically colonized/infected chronic leg ulcers. J Wound, Ostomy Cont Nurs. [Internet]. 2014;41(2):111-21. DOI: https://doi.org/10.1097/WON.0000000000000009
22. Heinen M, Borm G, Van der Vleuten C, Evers A, Oostendorp R, Van Achterberg T. The Lively Legs self-management programme increased physical activity and reduced wound days in leg ulcer patients: Results from a randomized controlled trial. Int J Nurs Stud. [Internet]. 2012;49(2):151-61. DOI: https://doi.org/10.1016/j.ijnurstu.2011.09.005
23. Kapp S, Miller C, Sayers V, Donohue L. The Leg Ulcer Prevention Program: effectiveness of a multimedia client education package for people with venous leg ulcers. Wound Pract Res [Internet]. 2010 May [cited 2019 Mar. 20];18(2):80. Available in: https://search.informit.com.au/documentSummary;dn=174647821217129;res=IELHEA
24. Van Hecke A, Grypdonck M, Beele H, Vanderwee K, Defloor T. Adherence to leg ulcer lifestyle advice: Qualitative and quantitative outcomes associated with a nurse-led intervention. J Clin Nurs. [Internet]. 2011;20(3-4):429-43. DOI: https://doi.org/10.1111/j.1365-2702.2010.03546.x
25. Finlayson KJ, Courtney MD, Gibb MA, O’Brien JA, Parker CN, Edwards HE. The effectiveness of a four-layer compression bandage system in comparison with Class 3 compression hosiery on healing and quality of life in patients with venous leg ulcers: A randomised controlled trial. Int Wound J. [Internet]. 2012;11(1):21-7. DOI: https://doi.org/10.1111/j.1742-481X.2012.01033.x
26. Wong IKY, Andriessen A, Charles HE, Thompson D, Lee DTF, So WKW, et al. Randomized controlled trial comparing treatment outcome of two compression bandaging systems and standard care without compression in patients with venous leg ulcers. J Eur Acad Dermatology Venereol. [Internet]. 2012;26(1):102-10. DOI: https://doi.org/10.1111/j.1468-3083.2011.04327.x
27. Edwards H, Courtney M, Finlayson K, Shuter P, Lindsay E. A randomised controlled trial of a community nursing intervention: Improved quality of life and healing for clients with chronic leg ulcers. J Clin Nurs. [Internet]. 2009;18(11):1541-9. DOI: https://doi.org/10.1111/j.1365-2702.2008.02648.x
28. Edwards H, Courtney M, Finlayson K, Lewis C, Lindsay E, Dumble J. Improved healing rates for chronic venous leg ulcers: Pilot study results from a randomized controlled trial of a community nursing intervention. Int J Nurs Pract. [Internet]. 2005;11(4):169–76. DOI: https://doi.org/10.1111/j.1440-172X.2005.00521.x
29. Edwards H, Kathleen F, Lindsay E, Patricia S, Allan C. Chronic Venous leg ulcers: Effect of a community nursing intervention on pain and healing. Nurs Stand. [Internet]. 2005;19(52):47-54. DOI: https://doi.org/10.7748/ns2005.09.19.52.47.c3950
30. Hoffmann TC, Glasziou PP, Barbour V, Macdonald H. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. Br Med J. [Internet]. 2014 Mar.;1-12. DOI: https://doi.org/10.1136/bmj.g1687
31. Meleis AI. Theoretical Nursing: Development and Progress. 5th Edit. Journal of Neuroscience Nursing. Wolters Kluwer Health. Lippincott Williams & Wilkins; 2012. 690 p.
32. Lindsay E. Lindsay leg clubs: Clinically effective, cost effective. J Community Nurs. [Internet] 2013 [cited 2019 Feb. 18];27(1):5-8. Available in: https://www.jcn.co.uk/journal/01-2013/wound-management/1529-lindsay-leg-clubs--clinically-effective--cost-effective/
33. Upton D, Upton P, Alexander R. Contribution of the Leg Club model of care to the well-being of people living with chronic wounds. J Wound Care [Internet]. 2015;24(9):397-405. DOI: https://doi.org/10.12968/jowc.2015.24.9.397
34. Lindsay E. Leg Clubs®: a clinically and cost-effective approach to lower limb management. Br J Community Nurs. [Internet]. 2014;15(Sup4:S16-23). DOI: https://doi.org/10.12968/bjcn.2010.15.Sup4.48379
35. Lindsay E. The Lindsay Leg Club Model: A model for evidence-based leg ulcer management. Br J Community Nurs. [Internet]. 2014; (Supplement: S15-20). DOI: https://doi.org/10.12968/bjcn.2004.9.Sup2.13128
36. Zajkowski PJÃ, Draper T, Bloom JÃ, Henke PKÃ, Wakefield TWÃ. Exercise with compression stockings improves reflux in patients with mild chronic venous insufficiency. Phlebology. [Internet]. 2006;21(2):9-13. DOI: https://doi.org/10.1258/026835506777304764
37. Araujo D, Riberiro C, Maciel A, Bruno S, Freonezi G, FAL D. Physical exercise for the treatment of non-ulcerated chronic venous insufficiency (review). Cochrane Database Syst Rev. [Internet]. 2016;3(12):1-35. DOI: https://doi.org/10.1002/14651858.CD010637.pub2
38. Orr L, Klement KA, Mccrossin L, Drombolis DO, Houghton PE, Spaulding S, et al. A systematic review and meta-analysis of exercise intervention for the treatment of calf muscle pump impairment in individuals with chronic venous insufficiency. Ostomy Wound Manag. [Internet]. 2017; 63(8):30-43. DOI: https://doi.org/10.25270/owm.2017.08.3043
39. Partsch H. Compression therapy in leg ulcers. Rev Vasc Med [Internet]. 2013;1(1):9-14. DOI: https://doi.org/10.1016/j.rvm.2013.02.001
40. O’Donnell TF, Passman MA, Marston WA, Ennis WJ, Dalsing M, Kistner RL, et al. Management of venous leg ulcers: Clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg. [Internet]. 2014;60(2):3S-59S. DOI: https://doi.org/10.1016/j.ejvs.2015.02.007
41. Raphael D, Waterworth S, Gott M. Telephone communication between practice nurses and older patients with long term conditions: a systematic review. J Telemed Telecare. [Internet]. 2017;23(1):142-8. DOI: https://doi.org/10.1177/1357633X15625398
42. Inglis SC, Clark RA, Cleland JG, McAlister F, Stewart S, Cleland J. Structured telephone support or telemonitoring programs for patients with chronic heart failure. Cochrane Database Syst Rev. [Internet]. 2010;(8):147. DOI: https://doi.org/10.1002/14651858.CD007228.pub2
43. Choi NG, Dinitto DM. The digital divide among low-income homebound older adults: Internet use patterns, ehealth literacy, and attitudes toward computer/internet use. J Med Internet Res. [Internet]. 2013;15(5):1-16. DOI: https://doi.org/10.2196/jmir.2645
44. Korda H, Itani Z. Harnessing social media for health promotion and behavior change. Health Promot Pract. 2013;14(1):15-23. DOI: https://doi.org/10.1177/1524839911405850
45. Segal J, Sacopulos M, Sheets V, Thurston I, Brooks K, Puccia R. Online doctor reviews: Do they track surgeon volume, a proxy for quality of care? J Med Internet Res. [Internet]. 2005;14(2):e50. DOI: https://doi.org/10.2196/jmir.2005
46. Skavberg Roaldsen K, Biguet G, Elfving B. Physical activity in patients with venous leg ulcer - between engagement and avoidance. A patient perspective. Clin Rehabil [Internet]. 2011;25(3):275-86. DOI: https://doi.org/10.1177/0269215510371424
47. Poku E, Aber A, Phillips P, Essat M, Buckley H, Palfreyman S, et al. Systematic review assessing the measurement properties of patient-reported outcomes for venous leg ulcers. BJS Open. [Internet]. 2017;1(5):138-47. DOI: https://doi.org/10.1002/bjs5.25
48. Walburn J, Vedhara K, Hankins M, Rixon L, Weinman J. Psychological stress and wound healing in humans: A systematic review and meta-analysis. J Psychosom Res. [Internet]. 2009;67(3):253-71. DOI: https://doi.org/10.1016/j.jpsychores.2009.04.002
49. Vegas O, VanBuskirk J, Richardson S, Parfitt D, Helmreich D, Rempel M, et al. Effects of psychological stress and housing conditions on the delay of wound healing. Psicothema. [Internet]. 2012;24(4):581-6. DOI: https://doi.org/10.1016/j.bbi.2008.04.043
50. Glaser R, Kiecolt-Glaser JK, Marucha PT, MacCallum RC, Laskowski BF, Malarkey WB. Stress-related changes in proinflammatory cytokine production in wounds. Arch Gen Psychiatry. [Internet]. 1999;56(5):450-6. DOI: https://doi.org/10.1001/archpsyc.56.5.450
51. Pieper B, Szczepaniak K, Templin T. Psychosocial adjustment, coping, and quality of life in persons with venous ulcers and a history of intravenous drug use. J Wound, Ostomy, Cont Nurs. [Internet]. 2000;27(4):227-37. DOI: https://doi.org/10.1067/mjw.2000.107877
52. Upton D, Solowiej K. Pain and stress as contributors to delayed wound healing. Wound Pract Res [Internet]. 2010 ausgust [cited 2019 Mar. 28];18(3):114-22. Available: https://search.informit.com.au/documentSummary;dn=364536431309445;res=IELHEA
53. Finlayson K, Miaskowski C, Alexander K, Liu W-H, Aouizerat B, Parker C, et al. Distinct wound healing and quality of life outcomes in subgroups of patients with venous leg ulcers with different symptom cluster experiences. J Pain Symptom Manage. [Internet]. 2017;53(5):871-9. DOI: https://doi.org/10.1016/j.jpainsymman.2016.12.336