Article
Sofia Almeida 1
Ana Nascimento2
Pedro Bernardes Lucas3
Élvio Jesus 4
Beatriz Araújo 5
1 ![]() 0000-0002-1874-0432. Universidade Católica do Porto, Center for
Interdisciplinary Health Research (CIIS), Portugal. spalmeida@porto.ucp.pt
0000-0002-1874-0432. Universidade Católica do Porto, Center for
Interdisciplinary Health Research (CIIS), Portugal. spalmeida@porto.ucp.pt
2 ![]() 0000-0001-6179-034X. Universidade Católica do Porto, Center for
Interdisciplinary Health Research (CIIS), Portugal. ananascimento@porto.ucp.pt
0000-0001-6179-034X. Universidade Católica do Porto, Center for
Interdisciplinary Health Research (CIIS), Portugal. ananascimento@porto.ucp.pt
3 ![]() 0000-0002-2560-7306. School of Nursing of Lisbon, Nursing Research and Development Unit, Portugal. prlucas@esel.pt
0000-0002-2560-7306. School of Nursing of Lisbon, Nursing Research and Development Unit, Portugal. prlucas@esel.pt
4 ![]() 0000-0002-8407-9240. Universidade Católica do Porto, Center for
Interdisciplinary Health Research (CIIS), Portugal. ejesus@porto.ucp.pt
0000-0002-8407-9240. Universidade Católica do Porto, Center for
Interdisciplinary Health Research (CIIS), Portugal. ejesus@porto.ucp.pt
5 ![]() 0000-0003-0266-2449. Universidade Católica do Porto, Center for
Interdisciplinary Health Research (CIIS), Portugal. baraujo@porto.ucp.pt
0000-0003-0266-2449. Universidade Católica do Porto, Center for
Interdisciplinary Health Research (CIIS), Portugal. baraujo@porto.ucp.pt
Received: 10/01/2020
Sent to peers: 28/02/2020
Approved by peers: 06/03/2020
Approved: 14/07/2020
Theme: Evidence-based practice
Contribution to the discipline: This paper presents a shorter version of the Practice Environment Scale of the Nursing Work Index (PES-NWI) for Portuguese nurses, with five dimensions, which constitutes a new solution for the Portuguese context. The validated version of the scale for Portuguese nurses can be used in several contexts (hospital centers, primary care); it is an essential tool for supporting decision-making and improving working conditions.
Para citar este artículo / To reference this article / Para citar este artigo: Almeida S, Nascimento A, Lucas PB, Jesus E, Araújo B. RN4CAST Study in Portugal: Validation of the Portuguese Version of the Practice Environment Scale of the Nursing Work Index. Aquichan. 2020;20(3):e2038. DOI: https://doi.org/10.5294/aqui.2020.20.3.8
|
Abstract Objective: This
study aims to validate the Portuguese version of the Practice Environment Scale
of the Nursing Work Index (PES-NWI) and assess construct validity through
exploratory and confirmatory factor analyses. Keywords (Source DeCS): Nursing; PES-NWI; psychometric properties; validation; working environment; surveys; questionnaires. |
Resumen Objetivo: este estudio tiene como
objetivo validar la versión portuguesa de la escala del entorno de práctica del
índice de trabajo de enfermería (PES-NWI, por sus siglas en inglés) y evaluar
la validez de los constructos mediante análisis factorial exploratorio
y confirmatorio. Palabras clave (Fuente DeCS): Enfermería; PES-NWI; propiedades psicométricas; validación; ambiente de trabajo; encuestas; cuestionarios. |
Resumo Objetivo: o objetivo deste estudo é validar a versão portuguesa
da escala do ambiente de prática do índice de trabalho de enfermagem (PES-NWI,
por sua sigla em inglês) e avaliar a validade dos constructos mediante análise
fatorial exploratória e confirmatória. Palavras-chave (Fonte DeCS): Enfermagem; escala PES-NWI; propriedades psicométricas; validação; ambiente de trabalho; questionários. |
Introduction
The Practice Environment Scale of the Nursing Work Index (PES-NWI) is an instrument that measures the nursing practice environment and is the most used worldwide. It was developed by Lake (1), who defines the nursing practice environment as “the organizational characteristics of a work setting that facilitate or constrain professional nursing practice” (1).
The PES-NWI has been translated and validated for several contexts worldwide and is applied to identify the organizational characteristics of the environments that are attractive to nurses. It was built through factor analysis of data from Magnet Hospitals (2) and is composed of subscales representing distinct domains of the nursing practice environment: Nurse Participation in Hospital Affairs (NPHA); Nursing Foundations for Quality of Care (NFQC); Nurse Manager Ability, Leadership and Support of Nurses (NMALSN); Staffing and Resource Adequacy (SRA); and Collegial Nurse-Physician Relations (CNPR) (1, 2).
From the perspective of Lake (1), favorable nursing practice environments are characterized by the adequacy of human and material resources, the active participation of nurses in organizations’ internal governance, the existence of nursing fundamentals for the quality of care, and the good relations among different professional groups, particularly doctors and nurses (3). In light of the scientific evidence in the last decades, such environments have significant impacts on the levels of quality and safety of user care, health workers’ well-being, and the quality, productivity, and effectiveness of health services, organizations, and systems. Thus, developing instruments to determine the quality of indicators that measure those work environments is necessary.
In Portugal, few studies have evaluated the practice environment and its implications. Nursing in the Portuguese context is associated with elevated stress, insufficient staff in the workplace, and poor recognition of professional nurses’ skills and experience (3). Amaral, Ferreira, and Lake (4) translated and validated the Portuguese PES-NWI, which retained the 31 items from the original version. However, the model revealed some limitations concerning its convergent, discriminant, and factorial validity, justifying the need for studies that adapt the PES-NWI to the Portuguese healthcare context. More studies could provide a different factor structure to obtain an adequate PES-NWI model to apply to the Portuguese nursing context. This study aims to validate the Portuguese version of the PES-NWI in the framework of the RN4CAST Portugal 2018 study and assess construct validity through exploratory and confirmatory factor analyses in a national sample of Portuguese nurses.
Materials and Methods
The study is methodological with a cross-sectional design to evaluate the psychometric properties of the PES-NWI in the Portuguese RN4CAST 2018 survey, which is a replication of the initial protocol.
It involved 5,075 nurses. The data sample covered 48 acute care hospitals (under the same administrative council), including three public-private partnerships and two private hospitals (primary health care centers and hospitals). The hospitals are located across the Portuguese continental territory and its autonomous regions, Madeira and the Azores. The sample was obtained through an online survey that was part of a broader research study (RN4CAST Portugal 2018). The participation of nurses was voluntary and anonymous. Nurses were included in the study regardless of their contractual relationship with the hospital (contractors or in-house staff). Nurses that were not practicing at the time of data collection were not considered. Data collection occurred between November 2017 and May 2018. The data was obtained from an online questionnaire with the following variables: demographic data (gender, age, educational background, marital status), and professional experience data (years of nursing practice experience and workplace.
The PES-NWI developed by Lake (1) was translated into Portuguese by Amaral, Ferreira, and Lake (4). It is composed of five subscales and 31 items that describe characteristics of practice nursing environments (1), which are rated on a Likert scale ranging from 1 (‘strongly agree’) to 4 (‘strongly disagree’). The original version comprises five domains that characterize practice environments: (a) NPHA, with nine items; (b) NFQC, with ten items; (c) NMALSN, with five items; (d) SRA, with four items; and (e) CNPR, with three items (1).
In the Portuguese version, Amaral, Ferreira, and Lake (4) keep the 31 items but has seven domains as a result of NPHA subdivision into Participation in Hospitals Affairs (PHA) with six items and Opportunities for Professional Development (OPD) with three items; and NFQC into Philosophy of Quality (PQ) with seven items and Continuity of Care (CC) with three items. The other dimensions of the scale had no changes (4). Lake (1) proposed the use of a mean score (set as 2.5) for each subscale and a composite measure as the average of the five subscale scores for data comparison among studies.
Statistical analyses
Continuous variables were described by mean and standard deviation, while categorical variables by absolute frequency and relative frequency. Statistical Package for the Social Sciences software (IBM® SPSS®, version 22.0) was used for descriptive analyses.
In the first stage, we performed an exploratory factorial analysis (EFA) with Varimax rotation to analyze the psychometric properties of the PES-NWI and identify its dimensions in a Portuguese national sample. The Kaiser-Meyer-Olkin (KMO) Measure of Sampling Adequacy was 0.909, while Bartlett’s test of Sphericity had a p-value < 0.001, indicating that the data were appropriate for factor analysis. For factor interpretation, items with a factor loading above 0.4 were retained. The Cronbach’s alpha was used to test internal consistency, considering values above 0.7 as acceptable.
In the second stage, using a subsample, we performed a confirmatory factorial analysis (CFA) to assess the instrument’s structure. We employed the IBM® AMOS software (25.0 version) to assess the model adjustment quality obtained from the EFA. The CFA was performed using the maximum likelihood method, which implies independence of observations, multivariate normality, and nonexistence of outliers. The normal distribution of the variables was analyzed using the skewness (Sk) and kurtosis (Ku) coefficients. Outliers were assessed using the squared Mahalanobis distance (D²) (5).
The goodness-of-fit index (GFI) was used to assess the global goodness-of-fit of the model. The comparative fit index (CFI), which scored above 0.90, revealed reasonable adjustment, and the root mean square error of approximation (RMSEA), with scores between 0.05 and 0.1, was acceptable. The model with the lowest modified expected cross-validation index (MECVI) shows proper adjustment; for this purpose, the modification indices predicted by AMOS and theoretical considerations were taken into account (5).
Convergent validity was assessed through the average variance extracted (AVE) with a minimum of 0.5 for each factor. Discriminant validity was considered good if the AVE of each factor was equal to or higher than the square of the correlations among the same factors (5).
Reliability and convergent validity of the adjusted model
Internal consistency was analyzed using Cronbach’s alpha (α). Construct validity was calculated using three sub-components. Convergent validity was calculated using the AVE for each factor and considering 0.50 as the minimum value for convergent validity. Discriminant validity was established when the AVE for both factors was equal to or greater than their squared correlation.
Results
Characteristics of hospitals and participants
Five thousand fifty-five nurses who work in mainland Portugal participated in this study. Most participants were female (72.6%), and 21.7% were male (Table 1). The nurses’ age varied between 22 and 66 years (M = 39.0; SD = 9.1); the mean worked as a nurse for 16.1 years. Most professionals (99.3%) had a degree in nursing, and 45.7% were specialists. Most nurses work in a hospital context (72.6%) and primary care (20.9%).
Table 1. Descriptive analysis of demographic variables of the study sample
n |
% |
Mean |
SD |
|
Gender |
||||
Female |
3,974 |
78.3 |
||
Male |
1,101 |
21.7 |
||
Age group |
||||
22–35 |
2,150 |
42.4 |
||
36–49 |
2,188 |
43.2 |
||
> 50 |
707 |
13.9 |
||
Workplace |
||||
Hospital context |
3,686 |
72.6 |
||
Primary care |
1,059 |
20.9 |
||
Integrated continuous care |
143 |
2.8 |
||
Residential structure for the elderly |
82 |
1.6 |
||
Other |
105 |
2.1 |
||
Degree in nursing |
||||
Yes |
5,041 |
99.3 |
||
Specialty in nursing |
||||
Yes |
2,318 |
45.7 |
||
Age (years) |
39.0 |
9.1 |
||
Years as a nurse |
16.1 |
9.1 |
||
SD: standard deviation
Source: Own elaboration.
The EFA of the PES-NWI identified five components that explain 54.6 % of the total variance. Items 14, 15, 18, and 19 did not respect the factor loading criteria and, for that reason, were excluded. The four excluded items were part of NFQC in the original version (1), and PQ in the Portuguese version (4). The final solution is composed of 27 items and five components (Table 2).
Table 2: Components of the Portuguese PES-NWI
NPHA |
SRA |
NMALSN |
NFQC |
CNPR |
|
4. Active staff development or continuing education programs for nurses |
0.562 |
||||
5. Career development/clinical ladder opportunity |
0.622 |
||||
6. Opportunity for staff nurses to participate in policy decisions |
0.606 |
||||
11. A chief nursing officer who is highly visible and accessible to staff |
0.469 |
||||
17. Opportunities for advancement |
0.614 |
||||
21. Management that listens and responds to employee concerns |
0.593 |
||||
22. An active quality assurance program |
0.568 |
||||
23. Staff nurses that are involved in the internal governance of the hospital |
0.667 |
||||
27. Opportunity for staff nurses to serve in hospital and nursing committees |
0.612 |
||||
28. Nursing managers that consult with staff on daily problems and procedures |
0.537 |
||||
25. A program with a mentor for newly hired nurses |
0.418 |
||||
1. Adequate support services to allow spending time with patients |
0.555 |
||||
8. Enough time and opportunity to discuss patient care problems with other nurses |
0.590 |
||||
9. Enough registered nurses to provide quality patient care |
0.863 |
||||
12. Enough staff to get the work done |
0.859 |
||||
3. A team of supervisors who support nurses |
0.511 |
||||
7. Mistakes used by supervisors as learning opportunities rather than criticism |
0.500 |
||||
10. A nurse manager who is a good manager and leader |
0.820 |
||||
13. Appreciation and recognition for the good accomplishment of a task |
0.443 |
||||
20. A nurse manager who backs up the nursing staff in decision-making, even in a conflict with a physician |
0.792 |
||||
26. Nursing care based on a nursing, not a medical model |
0.540 |
||||
29. Written, current nursing care plans for all patients |
0.768 |
||||
30. Patient care assignments that foster continuity of care, i.e., the same nurse takes care of the patient from one day to the next |
0.646 |
||||
31. Use of nursing diagnoses |
0.808 |
||||
2. Good working relationships between physicians and nurses |
0.793 |
||||
16. Much teamwork between nurses and physicians |
0.830 |
||||
24. Collaboration (joint practice) between nurses and physicians |
0.812 |
||||
Variance (%) |
31.1 |
7.1 |
6.3 |
5.6 |
4.5 |
Alpha |
0.862 |
0.779 |
0.816 |
0.730 |
0.813 |
Source: Own elaboration.
The five components identified are NPHA with 11 items, NMALSN with five items, SRA with four items, NFQC with four items, and NPR with three items. In the internal consistency analysis, the total scale had Cronbach’s alpha of 0.912, and, in the subscales, alpha was greater than 0.8, revealing excellent internal consistency.
The CFA was performed on the PES-NWI five-factor structure found in our sample. The PES-NWI items presented good factorial weights (> 0.3). Initially, the AFC model showed poor adjustment of the model (Χ2/df = 8,523; CFI = 0.851; RMSEA = 0.072). Additionally, the Mahalanobis distances indicated the presence of several multivariate outliers. Thus, we decided to remove some multivariate outliers from the model and analyze the modification indices. The PES-NWI model, without the five most severe outliers, also exhibited adjustment quality statistics that classify the model as suffering (Χ2/df = 8,552; CFI = 0.851; RMSEA = 0.072).
As the changes were not significant, we analyzed the model modification indices. The highest modification indices occurred in the correlations of errors: items 10 and 20, items 5 and 17, and items 23 and 27. The final model showed significantly better goodness-of-fit (Figure 1) with the sample under analysis and lower MECVI (1.06 vs. 1.70) than the original model. Adequate internal consistency and reproducibility of the total scale (α = 0.912) and subscales (Table 3) were observed. As an indicator of convergent validity, the AVE proved to be adequate for the NFQC and NPR factors (> 0.5), close to acceptable for the NMALSN and SRA factors, and low for the remaining factors. The analysis of the model’s factorial invariance in both independent subsets (test and validation) showed adequate goodness-of-fit indices in the final factor solution (χ2/df = 2,758.4; CFI = 0.91; GFI = 0.91; RMSEA = 0.056; MECVI = 1.15).
Figure 1. Five-factor model of the Portuguese PES-NWI
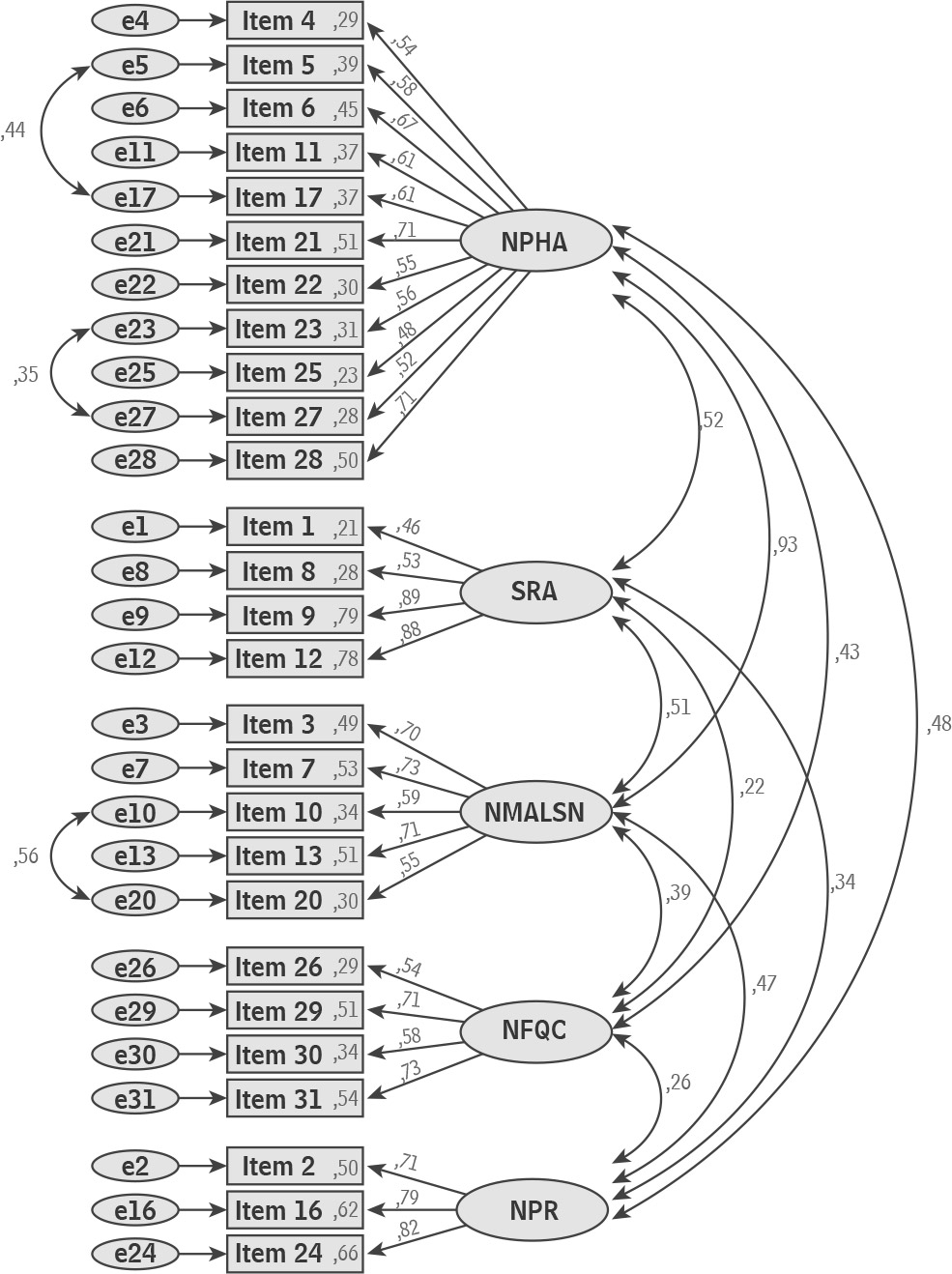
Source: Own elaboration.
Table 3. Construct validity analysis of the PES-NWI
Factors (5) |
AVE |
Nurse Participation in Hospital Affairs |
0.37 |
Nursing Foundations for the Quality of Care |
0.51 |
Nurse Manager Ability, Leadership and Support of Nurses |
0.46 |
Staffing and Resource Adequacy |
0.41 |
Collegial Nurse-Physician Relations |
0.60 |
Source: Own elaboration.
Discussion
The purpose of this study was to validate the Portuguese version of the PES-NWI in a national sample of Portuguese nurses, in the context of the RN4CAST Portugal 2018 study. It is the first study in the country to use a sample of Portuguese nurses who work in different health contexts to validate the PES-NWI.
Our results indicated a final 27-item structure and a five dimensions model, resulting in a different solution from that of the previous version validated in the Portuguese context (4). Our final study results for the PES-NWI matched three domains in the original version, SRA, NMALSN, and CNPR. The items excluded in our factorial analysis belong to the NFQC domain in the original version (1) and the PQ subscale in the Portuguese version (4).
In this study, we found a factorial structure with five components, which agrees with the one suggested by the author of the original scale (1). The CFA supported the five-factor model. The results are similar to other international studies (6–10).
The results from the EFA presented a five-dimension solution, which is like the original scale presented by Lake (1), but the items within the factors are different. In previous studies, similar variations in item structure have been observed (6–9). These can be due to differences in culture, health care systems, and management among countries, which may influence nurses’ responses.
EFA is a technique sensitive to sample size. It is important to note that the present study had a nationwide sample that was larger compared to the original version (n = 2299) (1), and more significant than the one used in the Portuguese context (n = 236) (4). This difference in sample sizes may contribute to different responses and the exclusion of most items within the NFQC domain.
The CFA model showed that the five-factor model fits well with the study sample in the Portuguese health context. The coefficients of the model’s goodness-of-fit indices were satisfactory. Nevertheless, the five-factor model showed good convergence, discriminant validity, and global internal consistency (α = 0.91) that was higher than the seven-factor model of Amaral, Ferreira, and Lake (4) (α = 0.83). The final model showed excellent reliability and construct validity, which supports the decision to exclude the items that are not essential to the construct being measured. Therefore, this shorter version of the PES-NWI can be used for future studies.
The invariance analysis of the five-factor model confirmed its stability. In our study, the internal consistency observed in the final five-factor model is higher than that obtained by Lake (1) (α = 0.82), Amaral, Ferreira, and Lake (4) (α = 0.89), and Fuentelsaz-Gallego, Moreno-Casbas, and González-María (8) (α = 0.90). The total scale and sub-scales of the five-factor model showed adequate reliability and internal consistency. Our results agree with those of other studies about the psychometric properties of the PES-NWI in different contexts (1, 4, 6, 10–15).
This methodological study has limitations. First, it administered a self-report questionnaire that cannot distinguish the influence of response biases. Second, it employed a non-random sampling technique that cannot distinguish between nurses working in private and public hospitals, which have critical organizational differences that could impact nurses’ perceptions of the work environment. This shorter version of the PES-NWI should be used in new studies and different work contexts to evaluate the nursing environment.
Conclusion
For the success of healthcare systems, the nursing work environment is critical; so, its measurement should be a regular practice available for both professionals and citizens to consult. This study contributed to the validation and psychometric property assessment of the Portuguese version of PES-NWI in a large sample at the national level. It also showed the adequate five-factor structure of the PES-NWI. The five-dimension model shows better specificity and stability in the analysis than the original version. Upon confirming this structure was reliable, all the factors showed adequate loading in their component and a semantic relationship among the items. This new model should be used in new studies to evaluate the work environment and improve healthcare conditions.
The validation of the Portuguese version of the PES-NWI in this study is a substantial contribution to the healthcare context; it is an essential tool in supporting decision-making, accessing the nursing environment, and improving working conditions.
Ethics approval and consent to participate: All participants were fully informed about the study, participated voluntarily, and had the right to withdraw at any time. Anonymity was maintained in all stages of the study. The Catholic University Committee of Ethics reviewed and approved the study’s protocol, which included the above ethical considerations (Process No. 3/2018).
Conflict of interests: None declared.
References
1. Lake ET. Development of the practice environment scale of the nursing work index. Res Nurs Health. 2002;25(3):176–188. DOI: https://doi.org/10.1002/nur.10032
2. Lake ET. The nursing practice environment: Measurement and evidence. Med Care Res Rev. [Internet]. 2007 [cited 2019 Dec 12];64(2 Suppl). DOI: https://doi.org/10.1177/1077558707299253
3. Jesus E, Roque, S, Amaral A. Estudo RN4CAST em Portugal: ambientes de prática de enfermagem. Rev Investig Enferm. 2015;13:26–44. Available from: http://hdl.handle.net/10400.14/19776
4. Amaral A, Ferreira PL, Lake ET. Validation of the Practice Environment Scale of the Nursing Work Index (PES-NWI) for the Portuguese nurse population. Int J Caring Sci. 2012;5(3):280–288. Available from: https://internationaljournalofcaringsciences.org/docs/7.%20%20Original%20Paper.pdf
5. Marôco J. Structural Equation Analysis: Theoretical Foundations, Software & Applications. 2nd ed. Pinheiro P, editor; 2014.
6. Alzate LCC, Bayer GLA, Squires A. Validation of a Spanish Version of the Practice Environment Scale of the Nursing Work Index in the Colombian Context. Hisp Health Care Int. [Internet]. 2014 [cited 2019 Dec 12];12(1):34–42. DOI: https://doi.org/10.1891/1540-4153.12.1.34
7. Choi J, Boyle DK. Differences in nursing practice environment among US acute care unit types: A descriptive study. Int J Nurs Stud. 2014;51(11):1441–1449. DOI: https://doi.org/10.1016/j.ijnurstu.2014.03.001
8. Fuentelsaz-Gallego C, Moreno-Casbas M, González-María E. Validation of the Spanish version of the questionnaire Practice Environment Scale of the Nursing Work Index. Int J Nurs Stud. 2013;50(2):274–280. DOI: https://doi.org/10.1016/j.ijnurstu.2012.08.001
9. Gasparino RC, Guirardello E. Validation of the Practice Environment Scale to the Brazilian culture. J Nurs Manage. 2017;25(5):375–383. DOI: https://doi.org/10.1111/jonm.12475
10. Mainz H, Baernholdt M, Ramlau-Hansen CH, Brink O. Comparison of nurse practice environments in Denmark and the USA. Int Nurs Rev. 2015;62(4):479–488. DOI: https://doi.org/10.1111/inr.12208
11. Neves TMA, Parreira P, Graveto J, Rodrigues V, Marôco J. Practice environment scale of the nursing work index: Portuguese version and psychometric properties. J Nurs Manage. 2018;26(7):1–9. DOI: https://doi.org/10.1111/jonm.12606
12. Parker D, Tuckett A, Eley R, Hegney D. Construct validity and reliability of the Practice Environment Scale of the Nursing Work Index for Queensland nurses. Int J Nurs Pract. 2010;16(4):352–358. DOI: https://doi.org/10.1111/j.1440-172X.2010.01851.x
13. Kirwan M, Matthews A, Scott PA. The impact of the work environment of nurses on patient safety outcomes: A multi-level modeling approach. International Journal of Nursing Studies. [Internet]. 2013 [cited 2019 Dec 12];50(2):253–263. DOI: https://doi.org/10.1016/j.ijnurstu.2012.08.020
14. Gabriel AS, Erickson RJ, Moran CM, Diefendorff JM, Bromley GE. A multilevel analysis of the effects of the practice environment scale of the nursing work index on nurse outcomes. Research in Nursing and Health. 2013;36(6):567–581. DOI: https://doi.org/10.1002/nur.21562
15. Swiger P, Patrician P, Miltner R, Raju D, Sproat S, Loan L. The Practice Environment Scale of the Nursing Work Index: An updated review and recommendations for use. Int J Nurs Stud. 2017;74:76–84. DOI: https://doi.org/10.1016/j.ijnurstu.2017.06.003