Introduction
Nursing professionals are highly susceptible to stressful life events. Due to the
nature of their profession, they experience suffering, uncertainty, and the loss of
patients 1,2, in addition to other sources of stress, such as interpersonal conflicts, excessive
demands, the constant need for technical-scientific and technological training, feelings
of devaluation, lack of professional autonomy and, often, unhealthy working conditions.
Furthermore, they experience a complex, multifaceted work routine permeated by stressors,
which exacerbates psychophysiological dysfunctions 2-5.
The autonomic nervous system (ANS) has a key role in the regulation of physiological
processes and the homeostatic balance of the human body. Neglected stress is one of
the main causes of ANS dysfunction and can trigger several psychological and physical
pathologies, such as depression, post-traumatic stress, burnout, and somatization
with cardiovascular, respiratory, and immunological repercussions, among others. As
a result, it negatively affects the professionals' health and, consequently, the performance
of their work activities 6-10.
Among the techniques used to assess and partially manage ANS, heart rate variability
(HRV) has emerged as a promising, non-invasive measure of autonomic balance, based
on photoplethysmography 7,11,12. HRV describes the oscillations in the interval between consecutive heartbeats (R-R
intervals within the QRS complex), as well as oscillations between consecutive, instantaneous
heart rates. Changes in HRV patterns provide a sensitive early indicator of health
impairment. Since low HRV rates often indicate abnormal and insufficient ANS adaptation,
this implies the presence of physiological dysfunction, which can be associated with
psycho-emotional disorders such as stress 10,12-14.
Cardiac coherence, one of the parameters of HRV, which is achieved when the heart
rhythm is in sync and resonance with the respiratory rhythm, ensures an increase in
the amplitude of heartbeat oscillations. Therefore, an increase in HRV rates indicates
good or sufficient adaptation of the ANS to the environment or a given stressful situation
12,15.
Cardiovascular biofeedback is an integrative and complementary mind-body practice
that uses breathing to control autonomic function. It also allows individuals to learn
how to modulate the body's response based on information from HRV. To this end, sensors
are placed next to the individual's body to monitor bodily functions and, simultaneously,
a computerized system translates this information into visual or sound signals that
provide feedback to the individual 11,12,16,17.
Cardiovascular biofeedback has been reported to be effective in treating various clinical
conditions and preventing and relieving symptoms related to physiological and subjective
stress. It also improves performance, especially in professionals whose work requires
efficient stress management, such as athletes, police officers, and managers 12,16,18,19. Studies on the use of biofeedback in nursing professionals and the benefits for
this group are still scarce, thus it is urgent to explore non-pharmacological tools
that can minimize the negative repercussions of stress and preserve these professionals'
homeostatic balance 20-23.
Based on the above, the objective is to verify the effectiveness of cardiovascular
biofeedback on the HRV parameters of nursing professionals working in a university
hospital, when compared to a computerized activity without self-monitoring.
Materials and Methods
Study Design and Location
This is a double-blind, parallel randomized clinical trial comparing two groups, conducted
from June 2020 to August 2021, with the Nursing Group of the Hospital de Clínicas de Porto Alegre, Brazil, an institution regarded as a reference center for health care and research
in Rio Grande do Sul. The study was conducted in line with the guidelines of the Consolidated
Standards of Reporting Trials (Consort).
Participants and Recruitment
The study population consisted of nursing professionals of both sexes, currently working
as nurses, who had been hired for over 90 days, considering the institutional legislation
regarding the validity of the probationary contract, working any shift scheduled at
the institution, allocated to the surgical nursing, clinical nursing, or clinical
inpatient nursing services, which have similar characteristics in terms of infrastructure,
organization, lighting, and the type of patient receiving care, not involve with the
hospitalization of patients with COVID-19 and with a general stress level greater
than 1 (GSL > 1).
The GSL was determined based on the Stress Symptom Scale. The scale's internal consistency
during validation was u = 0.92 for psychological symptoms and u = 0.90 for physical
symptoms. Based on the arithmetic mean of the items on this scale, the GSL was calculated,
where values greater than 1 indicate the presence of stress, ranging from 1.1 (lowest
stress) to 2.95 (maximum stress [24]).
The professionals excluded from the sample were those on long-term sick leave (social
security benefits and pregnancy or lactation leave) and vacation, or who returned
less than 15 days before their leave, professionals using pacemakers or who have heart
rhythm disorders (arrhythmia, tachycardia, and/or bradycardia).
The sample size calculation was estimated by the condition of interest -stress- and
based on a randomized clinical trial that showed a difference in stress levels immediately
after the intervention (Cohen's d = -0.33), as well as six weeks after implementing
the intervention (Cohen's d = -0.68 [25]). Considering a one-tailed sample with a
significance level of 5 %, power of 90 %, standardized effect size (Cohen's d) of
at least 0.4 between evaluations, and loss estimates of 5 % (no follow-up of participants
expected), a minimum sample of 57 professionals in the intervention group (IG) and
57 professionals in the control group (CG) was obtained, totaling 114 participants.
Participant Selection Logistics
The researchers randomly selected the participants, respecting the eligibility criteria,
based on the work schedules of each nursing service, using the "Name Draw" app for
Android®. The professionals selected were briefed on the study and received an informed
consent form, as well as the research protocol, consisting of questionnaires and scales
for measuring the variables of interest.
It is worth noting that the socio-occupational and health information questionnaire
was designed by the researchers to collect data on the participants' socio-biographical,
socio-occupational, health conditions, and self-reported previous illnesses.
Eligible professionals were randomized into IG and CG and then invited to participate
in the randomized clinical trial. Block randomization was decided via randomization.com,
which ensured that the number of participants was equally distributed in the groups.
Furthermore, it was conducted by one of the researchers who was not involved in performing
the activities with the participants to ensure that the sample was randomized.
Once the research subjects had provided their consent, the researcher or research
assistant scheduled the first appointment (t0). All procedures, regardless of the
allocation group, were conducted during the participant's working hours and in a private
location close to their work unit. Subjects were included in the study gradually,
from June 2020 to August 2021, until the minimum sample of 57 professionals per group
was reached.
Outcome
The outcome -improvement in HRV parameters- was evaluated by the root-mean-square
differences of successive R-R intervals (rMSSD), understood as the root mean square
difference of successive R-R intervals. The rMSSD is one of the parameters of the
HRV time domain and is measured in milliseconds (ms). It was also evaluated by cardiac
coherence - understood as the synchrony frequency between cardiac and respiratory
rhythms - which is one of the parameters of the frequency domain of HRV and is measured
in milliseconds per Hertz (ms/Hz). Both variables were measured using the HRV Assessment
module of the EmWave Pro Plus® software, developed and manufactured in the United States by Quantum Intech, Inc.
Boulder Creek, and designed by the Heart-Math Institute. This software uses a photoplethysmography
sensor, which is a reliable, valid, and accurate method for capturing and quantifying
physiological data related to the heartbeat in real time. It is the standard recommended
for analyzing HRV in the time and frequency domain 26.
The sensors were installed in the participants' earlobes and, regardless of whether
they were in the IG or CG, the HRV parameters were monitored and recorded as follows:
baseline measurement in the first appointment (t0) and measurement for five minutes
in the eight following appointments (from t1 to t8), performed after the activity
planned for the session according to the allocation group.
Intervention
The intervention consisted of training in the cardiovascular biofeedback technique,
using the interface and interactive games available in the EmWave Pro Plus® software. During the interactive game, based on the physiological behavior measured,
the software generates continuous and dynamic information allowing the participant
to gradually improve their respiratory and cardiac rhythm by maintaining the rhythm
and concentration with guided and standardized breathing 26.
Due to the peculiarities of the work routine of nursing professionals, the intervention
was divided into nine appointments, which were held three times a week for three weeks.
At t0, baseline HRV was measured, and instructions were provided on the dynamics of
the next appointments.
In the following IG appointments (from t1 to t8), guided deep breathing training was
provided, at a controlled and standardized rate, with the assistance of the York Biofeedback
Breath Pacer software (standardized "breathing" at six breaths per minute, 50/50 inhalation
ratio, with a pause after inhalation of 32 % and after exhalation of 20 %, prevalent
in 95 % of the population), combined with biofeedback, through interactive games provided
by the Em-Wave Pro Plus® software, lasting ten minutes per session. Participants were instructed on how to
perform guided deep breathing, as well as on the biofeedback data collected through
the sensor installed in the earlobe and viewed through the interface projected on
the computer screen for breathing self-modulation.
The control consisted of performing a computerized activity without self-monitoring
to keep the groups blinded. For this purpose, the Jigsaw Puzzles online application
was used, which consists of puzzles at varying levels of difficulty, which was played
on a tablet.
Every professional in the CG participated in the study for nine sessions. At t0, baseline
HRV was measured and in the following appointments, computerized activities were conducted
without self-monitoring, lasting ten minutes per session. EmWave Pro Plus® was also used, and the sensor was installed in the participant's ear-lobe, without
them being able to see the interface projected onto the computer screen. The equipment
was cleaned with a cloth soaked in 70 % isopropyl isopropyl alcohol before and immediately
after the activity.
To access and use the HRV monitoring system, interactive games, and their respective
evaluations, it was necessary to purchase photoplethysmography sensor devices via
the HeartMath Institute website: EmWave Ear Sensor and EmWave USB Sensor Module, and
licenses to download and access the full version of the EmWave Pro Plus® software, which was installed on laptop computers, in addition to completing a training
course. The York Biofeedback Breath Pacer respiratory stimulation system is available
to download and access free of charge on the York Biofeedback website.
Blinding and Data Collection Procedure
The participants were blinded to ensure that they were unaware of whether they were
being included in the IG or CG. The data collection instruments were self-administered
and handed to participants in a brown envelope. They were collected on a date agreed
upon by the participant and the researcher, and the data were double-entered into
Excel spreadsheets. The HRV data recorded by the software were compiled in Excel spreadsheets
at the end of each session and checked against the digitally saved records.
Due to the restriction on the number of research assistants because of the pandemic,
and the peculiarity of the activities in the groups, it was not possible to blind
the researchers and assistants who conducted the activities with the IG and CG. All
members of the research team were fully trained to maintain homogeneity in the approach,
guidance, and implementation of the proposed intervention.
Blinding was considered when analyzing the data. Hence, before the statistical consultancy,
the databases of both groups were unified and coded regarding the allocation of participants.
Statistical Analysis
The data were analyzed using the SPSS statistical package, version 20.0. The distribution
of continuous variables was assessed for normality using the Shapiro-Wilk test. Variables
with a normal distribution were compared using Student's t-test and, in the event
of asymmetry, the Mann-Whitney test was used. Pearson's Chi-squared or Fisher's exact
tests were used to compare proportions.
To assess the intervention's effect, considering that the measurements have been performed
three or more times, Generalized Estimating Equations [GEE] were employed, with multiple comparisons, and with Bonferroni's correction
(post hoc). The interaction's size was verified based on the difference mean (IG-CG) and on the
confidence interval (CI) between the groups. The effect size was calculated based
on Cohen's d.
Ethical Aspects
The present study was conducted in line with the ethical principles for research with
human beings. It is linked to a matrix project proposed by the Occupational Health
Interdisciplinary Team of the Universidade Federal do Rio Grande do Sul 20, registered in the Clinical Trials database, entitled "Biofeedback ef[f]ects on stress,
anxiety, and quality of professional life on [the] nursing staff of an (sic) university
hospital", under registration number NCT04446689, and approved by the Research Ethics
Committee of the Hospital de Clínicas de Porto Alegre, under ethics approval submission certificate number 23346619.0.0000.5327 and opinion
number 3.796.246.
Results
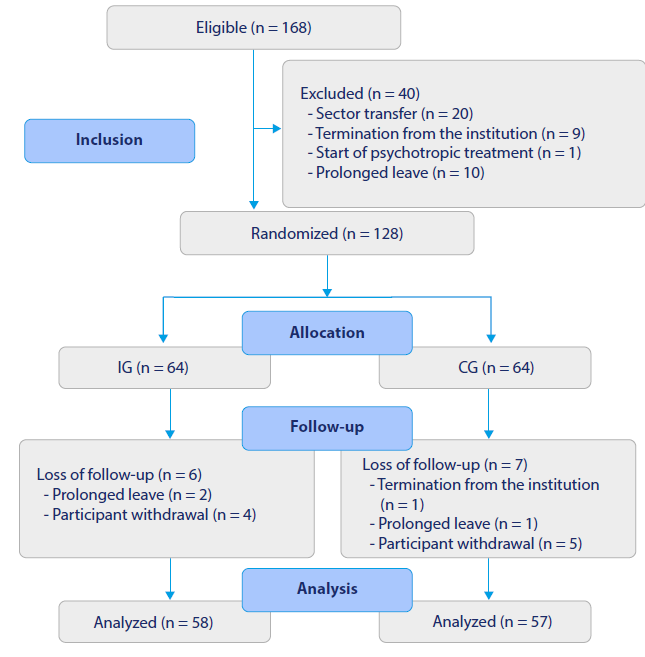
During the recruitment stage, 168 professionals showed stress symptoms. Reorganization
due to the COVID-19 pandemic regulations there were relocations, leaves, and terminations
of recruited professionals, which led to the exclusion of 40 professionals from the
sample.
Of the 128 professionals included and randomized into the IG and CG, six participants
in the IG and seven in the CG suffered follow-up losses. The analysis included a total
of 115 nursing professionals as detailed in the flowchart of the participants in the
study (Figure 1), developed in compliance with the Consort guidelines.
Figure 1
Flowchart of the Participants in the Study, in Line with the Consort Guidelines. Porto
Alegre, Rio Grande do Sul, 2021
Source: elaborated by the authors.
The participants' sociodemographic, occupational, and health characteristics are described
in Table 1. There were no statistically significant differences between the groups (p > 0.05),
indicating that the sample was homogeneous.
Table 1
Sociodemographic, Occupational, and Health Characteristics of IG and CG Participants.
Porto Alegre, Rio Grande do Sul, 2021
|
Characteristics |
IG
|
CG
|
p-value |
|
(n = 58)
|
(n = 57)
|
|
Age (years)*
|
42.2 ± 7.5
|
44.1 ± 9.3
|
0.235
|
|
Female**
|
47(81.0)
|
52(91.2)
|
0.190
|
|
Professional category**
|
|
|
0.993
|
|
Nurse
|
23(39.7)
|
22(38.6)
|
|
|
Nursing assistant
|
9(15.5)
|
9(15.8)
|
|
|
Nursing technician
|
26(45.6)
|
26(44.8)
|
|
|
Shift**
|
|
|
0.923
|
|
Morning
|
18(31.0)
|
21(36.8)
|
|
|
Afternoon
|
22(37.9)
|
19(33.3)
|
|
|
Night
|
13(22.4)
|
12(21.1)
|
|
|
Intermediate
|
05(8.8)
|
05(8.8)
|
|
|
Nursing experience (years)*
|
16.8 ± 6.7
|
18.3 ± 7.8
|
0.259
|
|
Single employment relationship**
|
50(86.2)
|
46(80.7)
|
0.587
|
|
Regularly used medication**
|
|
|
0.653
|
|
Antihypertensive(s)
|
6(10.3)
|
10(17.5)
|
|
|
Psychotropic(s)
|
11(19.0)
|
11(19.3)
|
|
|
Heartbeats per minute*
|
81 ± 1.5
|
79 ± 1.3
|
0.257
|
|
Practices physical activity**
|
29(50.0)
|
24(42.1)
|
0.508
|
|
Receives follow-up for psychological/ mental health**
|
12(20.7)
|
15(26.3)
|
0.623
|
|
Smoker**
|
6(10.3)
|
8(14.0)
|
0.749
|
|
24-hour sleep time*
|
6.6±1.5
|
6.8±1.4
|
0.299
|
|
Consumption of stimulating beverages (300ml or more per day)**
|
46(79.3)
|
41(71.9)
|
0.481
|
For detailing this study's results, the rMSSD and cardiac coherence parameters will
be analyzed exclusively for the effect of the time versus group interaction, since
comparisons between groups and between sessions (time) are not suitable for measuring
the effect of the intervention.
Table 2 displays the effect of the cardiovascular biofeedback intervention on rMSSD. The
GEE results show that there was no significant time-group interaction for rMSSD (p
= 0.432) at any of the measurement times. It should be noted that, although not statistically
significant, the mean difference of the interaction was considerably higher for the
IG at t3, with an increase of 14.07 points in rMSSD compared to the CG (p = 0.323).
Furthermore, in the two following intervention sessions (t4 and t5), the IG presented
a reduction of -8.22 and -11.21 points respectively in the rMSSD compared to the CG
(p = 0.568 and p = 0.241).
Table 2
Description of the rMSSD mean in the IG and CG, and the effect of the interaction
between time and group in each session (t). Porto Alegre, Rio Grande do Sul, Brazil,
2021
|
Session
|
rMSSD
|
|
IG*
|
CG*
|
Time-Group Interaction**
|
p-value
|
|
Mdif
|
CIdif 95 %
|
|
t0
|
49.8 ± 4.3
|
47.1 ± 4.0
|
2.76
|
-08.78 - 14.29
|
0.639
|
|
t1
|
65.7 ± 8.6
|
58.1 ± 6.5
|
7.60
|
-13.55 - 28.76
|
0.481
|
|
t2
|
61.8 ± 5.9
|
58.1 ± 6.9
|
3.67
|
-14.10 - 21.45
|
0.686
|
|
t3
|
82.0 ± 12.2
|
67.9 ± 7.3
|
14.07
|
-13.85 - 41.99
|
0.323
|
|
t4
|
70.5 ± 9.7
|
78.7 ± 10.6
|
-8.22
|
-36.40 - 19.96
|
0.568
|
|
t5
|
56.2 ± 5.0
|
67.4 ± 8.1
|
-11.21
|
-29.97 - 07.54
|
0.241
|
|
t6
|
66.4 ± 7.0
|
65.3 ± 7.9
|
1.05
|
-19.70 - 21.79
|
0.921
|
|
t7
|
64.6 ± 7.7
|
67.5 ± 9.8
|
-2.85
|
-27.33 - 21.62
|
0.819
|
|
t8
|
73.3 ± 10.9
|
72.4 ± 11.0
|
0.95
|
-29.45 - 31.33
|
0.952
|
Table 3 shows the effect of the cardiovascular biofeedback inter- vention on cardiac coherence.
The GEE results indicate that there was a significant time-group interaction for cardiac
coherence (p < 0.002) at all measurement times. It is worth noting that the means
for the difference (interaction size) showed a considerable increase after the first
training session with cardiovascular biofeedback (t1), in which the IG showed an increase
of 28.10 points in cardiac coher- ence when compared to the CG (p < 0.001), with a
large effect size (Cohen’s d = 14.86; r = 0.99). The greatest interaction effect occurred
at t5 when the IG showed a 30.18-point increase in cardiac coher- ence rates compared
to the CG (p < 0.001; Cohen’s d = 17.71; r = 0.99). Excluding the baseline measurement
(t0), the smallest interaction size occurred after the last cardiovascular biofeedback
training ses- sion (t8), in which the IG showed a 25.62-point increase in cardiac
coherence compared to the CG (p < 0.001); still, with a large effect size (Cohen’s
d = 13.79; r = 0.98).
Table 3
Description of the Mean Cardiac Coherence in the IG and CG and the Effect of the Interaction
between Time and Group in each Session (t). Porto Alegre, Rio Grande do Sul, Brazil,
2021
|
Session
|
Cardiac coherence
|
|
IG*
|
CG*
|
Time-Group Interaction**
|
p-value
|
|
Mdif
|
CIdif 95 %
|
|
t0
|
43.8 ± 2.1
|
35.8 ± 1.5
|
8.04
|
02.89 - 13.18
|
0.002
|
|
t1
|
64.5 ± 2.3
|
36.4 ± 1.4
|
28.10
|
22.84 - 33.35
|
<0.001
|
|
t2
|
62.1 ± 2.4
|
34.2 ± 1.0
|
27.82
|
22.70 - 32.94
|
<0.001
|
|
t3
|
62.4 ± 2.6
|
33.7 ± 1.2
|
28.70
|
23.16 - 34.23
|
<0.001
|
|
t4
|
61.0 ± 2.4
|
32.4 ± 1.4
|
28.65
|
23.22 - 34.08
|
<0.001
|
|
t5
|
63.7 ± 2.1
|
33.6 ± 1.2
|
30.18
|
25.41 - 34.95
|
<0.001
|
|
t6
|
60.2 ± 2.3
|
34.3 ± 1.1
|
25.89
|
20.75 - 31.03
|
<0.001
|
|
t7
|
59.5 ± 2.4
|
32.7 ± 1.1
|
26.83
|
21.60 - 32.07
|
<0.001
|
|
t8
|
59.5 ± 2.4
|
33.9 ± 1.1
|
25.62
|
20.36 - 30.88
|
<0.001
|
Discussion
The effectiveness of the intervention with cardiovascular biofeedback in improving
the cardiac coherence parameters of nursing professionals working in hospital sectors
was found in this study, which was evaluated using the EmWave Pro Plus® HRV Assessment module.
The time-group interaction showed that cardiac coherence rates presented a statistically
significant increase in the IG when compared to the CG, with a large effect size at
all measurement times, as well as a tendency towards stability during the follow-up
period.
This result corroborates those of previous studies conducted with different populations
12,27 and replicates the foundational relationship between cardiac coherence and emotions
8 since an increase in cardiac coherence biomarkers is associated with the use of tools
for respiratory modulation and, consequently, for the physiological relaxation response.
In a study conducted in France, healthy individuals were exposed to a period of stress
and then either practiced biofeedback techniques (n = 15) or watched a neutral video
(n = 14). The results showed that biofeedback is a proactive and relevant tool for
coping with stress. Compared to the group that watched the video, participants who
practiced biofeedback achieved higher cardiac coherence scores and medium effect size
(F 2,33 = 28.34, p < 0.001, T]2 = 0.63). Post-intervention self-reported measurements
showed that biofeedback contributed to reducing self-perceived psychological stress
and increasing perceived levels of performance. In addition, participants estimated
that 11 (± 5) minutes of biofeedback intervention was ideal for coping with an upcoming
stressful event, promoting relaxation and better coping, among other positive effects
for ANS balance 27.
The data presented in the paragraph above, although related to a study conducted with
the French population 27, are similar to those found in the present study, which was conducted with nursing
professionals who presented stress symptoms and in which the intervention with cardiovascular
biofeedback showed a large effect size at all measurement times when compared to the
placebo activity (p < 0.001; Cohen's d >13.79; r > 0.98).
The psychophysiological state of cardiac coherence, achieved when the heart rate accelerates
and decelerates in harmony with the respiratory rate, contributes to positive changes
in HRV and blood pressure, activating the body's regulatory and cyclical functions,
such as the endocrine and neuroimmunological systems. Positive physiological changes,
seen when individuals reach this state of synchrony and maintain it through breathing
self-control, promote a lasting condition of ANS balance and emotional stability 12,27.
In this study, the effectiveness of the intervention with cardiovascular biofeedback
on the rMSSD parameters of the participating professionals could not be supported
by the assessments using the EmWave Pro Plus® HRV Assessment module. Although at some points considerable mean differences were
found in the interaction, these were not statistically significant in the time-group
interaction. In fact, the participants' rMSSD behavior in both groups oscillated.
An equivalent result was reported in a previous study 27 conducted with healthy French individuals, in which rMSSD scores showed no statistically
significant effect between the IG and CG (x2 = 1.21, p = 0.27). In a meta-analysis
conducted to analyze studies that justified selecting HRV as a psychological stress
indicator, the authors found that the most frequently reported factor associated with
variation in HRV variables was low parasympathetic activity 7.
However, it is worth understanding that although rMSSD quantifies ANS parasympathetic
activity, in which passive relaxation responses and homeostasis recovery prevail,
the data analyzed in the present study (rMSSD) provides the quantification of short-term
variations in parasympathetic activation. Considering that, among other functions,
the parasympathetic system reduces heart rate, it is clear that the oscillations in
parasympathetic short-term variations do not reflect something negative, but possibly
their action in opposition to sympathetic activity 8. Among the participants in this randomized clinical trial, this activation occurred
in the bodies of individuals who self-reported stress and were learning to modulate
their breathing to regain their psychophysiological balance.
Therefore, in line with studies conducted with different populations 7,27, cardiovascular biofeedback can be considered a promising tool, in light of the physiological
and psychological effects found in improving cardiac coherence, as well as in activating
the parasympathetic system. In this study, these effects were achieved even without
intensive training and with a standardized protocol for guided deep breathing.
Furthermore, as a mind-body therapy, cardiovascular biofeedback has proven to be a
promising and useful tool in specific situations since, by promoting parasympathetic
activation and relaxation, it can enable the prevention of a range of deleterious
effects associated with occupational stressors 14,16. In just ten minutes of cardiovascular biofeedback training, the nursing professionals
participating in the IG learned how to modulate consciously and partially their body's
responses, recovering ho-meostasis, as well as enabling self-knowledge and self-awareness
of their feelings and emotions, according to physiological or pathological behaviors,
minimizing the negative effects of occupational stressors.
It is worth considering that the study was conducted during the nurses' professional
practice and, although the participants were not providing direct care to COVID-19
patients, they were experiencing the impacts and uncertainties stemming from the pandemic
in their daily family, social, and organizational lives.
In this sense, the following limitations were identified: The inability to individualize
the controlled frequency and/or resonant frequency for guided deep breathing training,
due to the standardization of the activities performed to minimize bias in the research,
in line scientifically recommended methodological principles; in addition, the logistics
of the sessions, which, due to the work routine of the nursing team, were not conducted
consecutively.
Conclusion
The intervention with cardiovascular biofeedback proved to have a greater effect than
the placebo in improving the nursing professionals' cardiac coherence rates, whose
physiological data were assessed using the EmWave Pro Plus® HRV Assessment module, which is reflected in the recovery of the body's homeostasis.
There was no statistical evidence of an improvement in the rMSSD parameters, which
quantify short-term variations in the parasympathetic activation of the ANS, in the
participating nursing professionals.
