Introduction
The discussion on palliative care (PC) has progressed as a result of demographic changes,
disease patterns, and the number of people living with chronic conditions with no
prospect of recovery 1,2. The need for comprehensive care that supports strategies for addressing life-threatening
illnesses renders this approach extremely necessary, especially in terms of hospitalization
in high-tech and interventional environments, such as the perioperative setting to
redefine praxis in a reality with a reserved prognosis 3.
In the surgical setting, which is highly complex and requires hard technologies, palliation
should be understood as an innovative, humanized approach focused on the concepts
of comfort and suffering relief; it should never be understood as diverging from or
opposing conventional perioperative practice 4-6. On the contrary, this strategy should be complementary to surgery, and, in turn,
surgery should support palliation to provide comfort and optimize the patient's well-being.
7,8.
In this sense, it should be noted that surgical culture and PC are not mutually exclusive,
nor are they sequential 5. Even if all the anxiety and hope of patients who undergo surgery regarding their
recovery is factored in, the dissolution of platitudes concerning the exclusivity
of one practice or another is imperative in an attempt to establish full, quality
care, especially for the elderly, who are the most demanding population in terms of
PC, due to their susceptibility and the coexistence of morbidities. 9,10.
Individuals over the age of 60 who have two or more associated co-morbidities comprise
the percentage of the population that needs hospitalization the most in the last year
of life, with a high probability of undergoing surgical procedures 11,12. In a broad overview, data from MediCare, the US health insurance system, estimates
that 500,000 elderly people in the United States alone undergo high-risk surgery,
with a mortality rate of approximately 20 %. 13.
It was estimated that of the 5,411,087 surgeries performed by the Unified Health System
in Brazil in 2022, approximately 40 % were performed on elderly patients 14,15. Regarding elective surgeries, multimorbidities are the main underlying causes for
these procedures, with special emphasis on neoplasms and malignant tumors, which are
the second leading cause of mortality among the elderly in Latin America, the European
Union, and the USA, only behind cardiocirculatory diseases 2,12,16.
Procedures such as tracheostomy and percutaneous endoscopic gastrostomy are routine
treatments that relieve the symptoms of esophageal cancer, head and neck cancer, and
amyotrophic lateral sclerosis 5,11. Intestinal detour surgeries and colostomies are performed to relieve malignant intestinal
obstruction and palliative amputations are common in vascular surgery 5,11,12.
Despite the unquestionable organic stress imposed on individuals over the age of 60
as a result of such a procedure, surgeries, when well prescribed, provide unparalleled
comfort and relief 6,17. Therefore, the challenge lies in the complexity of implementing and integrating
PC into the perioperative process, enabling them to juxtapose these approaches early
on, with special emphasis on nursing, in its role as a protagonist, whether in providing
care that aims to identify patients in need of palliation, or in developing care that
provides dignity, based on strategies and, above all, being empathetic and humane
3,18.
For nurses, PC includes aggressive management of pain and symptoms, psychological,
social, and spiritual support, as well as discussions concerning advanced care planning,
which can include decision-making about treatment and coordination of complex care
19. Specialized PC for surgical elderly patients, provided by a trained nursing team,
can help manage complex symptoms, provide additional support to families, solve conflicts
in treatment objectives and approaches, and assist in care transition 18.
To this end, it is necessary to understand and know the nursing actions and care -pre-,
trans-, or post-operative- provided to these patients in wards or intensive care units
(ICUs), and, therefore, understand the challenges involved in the implementation of
this process, as well as whether the provision of care occurs empirically or systematically,
whether it is frequent or infrequent, and what dimensions are involved in this process.
It is essential, thus, that in a perioperative hospitalization setting, such as the
one discussed here, the professional nurse should not only be the one who structures
patient care, but also the one who is responsible for welcoming, addressing, and alleviating
biophysical and psychological suffering 20,21.
Hence, this scoping review aimed to map and identify the existing works in the literature
on nursing actions focused on palliative care for the elderly in a surgical hospitalization
setting, considering the intrinsic relationship between the aging phenomenon, illness
processes, the need for surgical procedures, and the establishment of palliative care
by the nursing team. This study not only helps to elucidate the role of the profession
but is also justified by the inherence and pertinence of a widespread, common, but
scarcely addressed theme, in an attempt to improve efforts to provide comfort and
quality of care.
Materials and Methods
This is a descriptive, exploratory, scoping review, based on a specific manual proposed
by the Joanna Briggs Institute 22, using the Preferred Reporting Items for Systematic Review tool, with its extension
for scoping reviews (Prisma-ScR). This method allows the main concepts to be mapped,
research areas to be clarified, and knowledge gaps to be identified (Figure 1).
Figure 1
PRISMA-ScR Flowchart for the Study Search and Selection Process
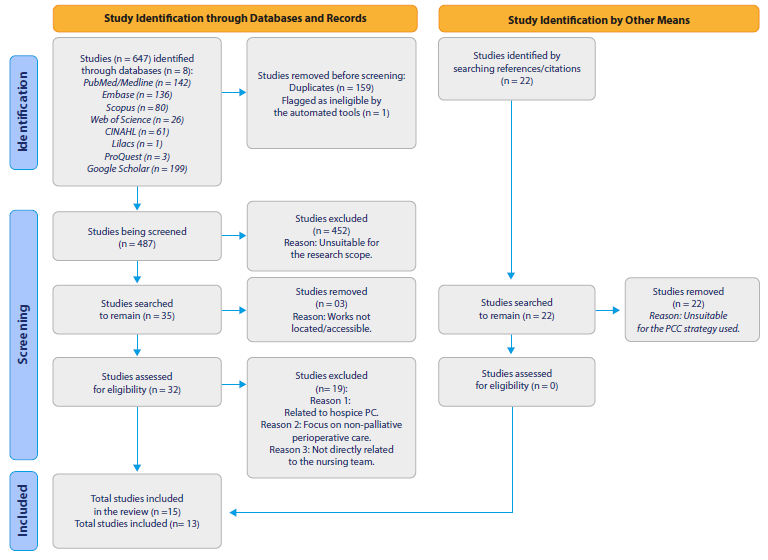
Source: Elaborated by the authors.
The research stages were the following: i) development of the research question; ii)
inclusion and exclusion criteria selection; iii) identification of key terms; iv)
identification of databases; v) study selection, and vi) mapping the articles and
reporting the results.
The "population, concept, context" (PCC) strategy was used to develop this study,
which includes the following eligibility criteria: for the population - elderly people who meet the WHO definition of elderly (65 years) or the Elderly
Statute (60 years, in the Brazilian context [23,24]); concept - PC is defined as care provided by a multidisciplinary team, which aims to improve
the quality of life of patients and their families facing a life-threatening illness,
through the prevention and relief of suffering, early identification, impeccable assessment
and treatment of pain and other physical, social, psychological, and spiritual symptoms
(WHO [25]). Regarding the context - studies referring to elderly people in perioperative circumstances were included.
Thus, only productions that specifically included PC nursing interventions for elderly
patients in perioperative settings were included.
To guide the collection of scientific evidence, the following question was asked:
What are the nursing actions/care provided to elderly people receiving PC in a surgical
hospitalization setting?
The search was conducted independently by two researchers and a reviewer in June 2023,
and the results were then compared and merged into a single database provided by the
Rayyan® software. However, data was first collected from the Medline/PubMed database by testing
MeSH terms and index terms (Table 1). Following this step, the search strategy was completed and implemented in the other
databases used in the review, according to the particularities of each one, which
was coordinated by a professional librarian.
Table 1
Databases and Search Strategies
|
Database
|
Search strategy
|
Results June 2023
|
|
Medline/ PubMed
|
(“Nursing Care”[MeSH Terms] OR “Nursing Care”[All Fields] OR “nursing interventions”[All
Fields] OR “nursing intervention”[All Fields] OR “Nursing”[MeSH Terms] OR “Nursing”[All
Fields]) AND (“Aged”[MeSH Terms] OR “Aged”[All Fields] OR “Elderly”[All Fields] OR
“aged, 80 and over”[MeSH Terms] OR “80 and over”[All Fields] OR “Oldest Old”[All Fields]
OR “Nonagenarian”[All Fields] OR “Nonagenarians”[All Fields] OR “Octogenarians”[All
Fields] OR “Octogenarian”[All Fields] OR “Centenarians”[All Fields] OR “Centenarian”[All
Fields] OR “geriatric”[All Fields] OR “Middle Aged”[MeSH Terms] OR “Middle Aged”[All
Fields] OR “Middle Age”[All Fields]) AND (“Palliative Care”[MeSH Terms] OR “Palliative
Care”[All Fields] OR “Palliative Treatment”[All Fields] OR “Palliative Treatments”[All
Fields] OR “Palliative Therapy”[All Fields] OR “Palliative Supportive Care”[All Fields]
OR “Palliative Surgery”[All Fields] OR “Palliative Medicine”[MeSH Terms] OR “Palliative
Medicine”[All Fields] OR “Hospice and Palliative Care Nursing”[MeSH Terms] OR “Hospice
and Palliative Care Nursing”[All Fields] OR “Palliative Nursing”[All Fields] OR “Palliative
Care Nursing”[All Fields] OR “Hospice Nursing”[All Fields] OR “Hospice Care”[MeSH
Terms] OR “Hospice Care”[All Fields] OR “Hospice Programs”[All Fields] OR “Hospice
Program”[All Fields] OR “Bereavement Care”[All Fields] OR “Terminal Care”[MeSH Terms]
OR “Terminal Care”[All Fields] OR “End of Life Care”[All Fields] OR “End of Life Cares”[All
Fields] OR “Hospices”[MeSH Terms] OR “Hospices”[All Fields] OR “Hospice”[All Fields]
OR “Critical Illness”[MeSH Terms] OR “Critical Illness”[All Fields] OR “Critical Illnesses”[All
Fields] OR “Critically Ill”[All Fields]) AND (“Perioperative Period”[MeSH Terms] OR
“Perioperative Period”[All Fields] OR “Perioperative Periods”[All Fields] OR “Perioperative
Care”[MeSH Terms] OR “Perioperative Care”[All Fields] OR “Surgical patients”[All Fields]
OR “Surgical patient”[All Fields])
|
142
|
|
Embase
|
(‘nursing care’/de OR ‘nursing care’ OR ‘nursing interventions’ OR ‘nursing intervention’/de
OR ‘nursing intervention’ OR ‘nursing’/de OR nursing) AND (‘aged’/de OR aged OR ‘elderly’/
de OR elderly OR ‘80 and over’ OR ‘oldest old’ OR ‘nonagenarian’/de OR nonagenarian
OR ‘nonagenarians’/de OR nonagenarians OR ‘octogenarians’/de OR octogenarians OR ‘octogenarian’/
de OR octogenarian OR ‘centenarians’/de OR centenarians OR ‘centenarian’/de OR centenarian
OR ‘geriatric’/de OR geriatric OR ‘middle aged’/de OR ‘middle aged’ OR ‘middle age’/de
OR ‘middle age’) AND (‘palliative care’/de OR ‘palliative care’ OR ‘palliative treatment’/de
OR ‘palliative treatment’ OR ‘palliative treatments’ OR ‘palliative therapy’/de OR
‘palliative therapy’ OR ‘palliative supportive care’ OR ‘palliative surgery’/de OR
‘palliative surgery’ OR ‘palliative medicine’/de OR ‘palliative medicine’ OR ‘hospice
and palliative care nursing’/de OR ‘hospice and palliative care nursing’ OR ‘palliative
nursing’/de OR ‘palliative nursing’ OR ‘palliative care nursing’/de OR ‘palliative
care nursing’ OR ‘hospice nursing’/de OR ‘hospice nursing’ OR ‘hospice care’/de OR
‘hospice care’ OR ‘hospice programs’ OR ‘hospice program’ OR ‘bereavement care’/de
OR ‘bereavement care’ OR ‘terminal care’/de OR ‘terminal care’ OR ‘end of life care’/de
OR ‘end of life care’ OR ‘end of life cares’ OR ‘hospices’/de OR hospices OR ‘hospice’/de
OR hospice OR ‘critical illness’/de OR ‘critical illness’ OR ‘critical illnesses’
OR ‘critically ill’/de OR ‘critically ill’) AND (‘perioperative period’/de OR ‘perioperative
period’ OR ‘perioperative periods’ OR ‘perioperative care’/de OR ‘perioperative care’
OR ‘surgical patients’ OR ‘surgical patient’/de OR ‘surgical patient’)
|
136
|
|
Scopus
|
TITLE-ABS-KEY(“Nursing Care” OR “nursing interventions” OR “nursing intervention”
OR nursing) AND TITLE-ABS-KEY(Aged OR Elderly OR “80 and over” OR “Oldest Old” OR
Nonagenarian OR Nonagenarians OR Octogenarians OR Octogenarian OR Centenarians OR
Centenarian OR geriatric OR “Middle Aged” OR “Middle Age”) AND TITLE-ABS-KEY(“Palliative
Care” OR “Palliative Treatment” OR “Palliative Treatments” OR “Palliative Therapy”
OR “Palliative Supportive Care” OR “Palliative Surgery” OR “Palliative Medicine” OR
“Hospice and Palliative Care Nursing” OR “Palliative Nursing” OR “Palliative Care
Nursing” OR “Hospice Nursing” OR “Hospice Care” OR “Hospice Programs” OR “Hospice
Program” OR “Bereavement Care” OR “Terminal Care” OR “End of Life Care” OR “End of
Life Cares” OR Hospices OR Hospice OR “Critical Illness” OR “Critical Illnesses” OR
“Critically Ill”) AND TITLE-ABS-KEY(“Perioperative Period” OR “Perioperative Periods”
OR “Perioperative Care” OR “Surgical patients” OR “Surgical patient”)
|
80
|
|
Web of Science
|
TS=(“Nursing Care” OR “nursing interventions” OR “nursing intervention” OR nursing
) AND TS=(Aged OR Elderly OR “80 and over” OR “Oldest Old” OR Nonagenarian OR Nonagenarians
OR Octogenarians OR Octogenarian OR Centenarians OR Centenarian OR geriatric OR “Middle
Aged” OR “Middle Age”) AND TS=(“Palliative Care” OR “Palliative Treatment” OR “Palliative
Treatments” OR “Palliative Therapy” OR “Palliative Supportive Care” OR “Palliative
Surgery” OR “Palliative Medicine” OR “Hospice and Palliative Care Nursing” OR “Palliative
Nursing” OR “Palliative Care Nursing” OR “Hospice Nursing” OR “Hospice Care” OR “Hospice
Programs” OR “Hospice Program” OR “Bereavement Care” OR “Terminal Care” OR “End of
Life Care” OR “End of Life Cares” OR Hospices OR Hospice OR “Critical Illness” OR
“Critical Illnesses” OR “Critically Ill”) AND TS=(“Perioperative Period” OR “Perioperative
Periods” OR “Perioperative Care” OR “Surgical patients” OR “Surgical patient”)
|
26
|
|
CINAHL
|
(“Nursing Care” OR “nursing interventions” OR “nursing intervention” OR nursing) AND
(Aged OR Elderly OR “80 and over” OR “Oldest Old” OR Nonagenarian OR Nonagenarians
OR Octogenarians OR Octogenarian OR Centenarians OR Centenarian OR geriatric OR “Middle
Aged” OR “Middle Age”) AND (“Palliative Care” OR “Palliative Treatment” OR “Palliative
Treatments” OR “Palliative Therapy” OR “Palliative Supportive Care” OR “Palliative
Surgery” OR “Palliative Medicine” OR “Hospice and Palliative Care Nursing” OR “Palliative
Nursing” OR “Palliative Care Nursing” OR “Hospice Nursing” OR “Hospice Care” OR “Hospice
Programs” OR “Hospice Program” OR “Bereavement Care” OR “Terminal Care” OR “End of
Life Care” OR “End of Life Cares” OR Hospices OR Hospice OR “Critical Illness” OR
“Critical Illnesses” OR “Critically Ill”) AND (“Perioperative Period” OR “Perioperative
Periods” OR “Perioperative Care” OR “Surgical patients” OR “Surgical patient”)
|
61
|
|
Lilacs
|
(“Nursing Care” OR “nursing interventions” OR “nursing intervention” OR nursing OR
“Cuidados de Enfermagem” OR “Cuidado de Enfermagem” OR “Assistência de Enfermagem”
OR “Atendimento de Enfermagem” OR “Atención de Enfermería” OR “Cuidado de Enfermería”
OR “Cuidados de Enfermería” OR enfermeiros OR enfermeiras OR enfermeras OR enfermeros
OR enfermagem OR enfermería) AND (aged OR elderly OR “80 and over” OR “Oldest Old”
OR nonagenarian OR nonagenarians OR octogenarians OR octogenarian OR centenarians
OR centenarian OR geriatric OR “Middle Aged” OR “Middle Age” OR idoso OR idosos OR
idosa OR idosas OR “Pessoa de Idade” OR “Pessoas de Idade” OR anciano OR ancianos
OR “Adulto Mayor” OR “Persona Mayor” OR “Persona de Edad” OR “Personas Mayores” OR
“Personas de Edad” OR “Idoso de 80 Anos ou mais” OR centenarios OR nonagenarios OR
octogenarios OR velhíssimos OR “Anciano de 80 o más Años” OR viejísimos OR geriátrico
OR geriátricos OR geriátrica OR geriátricas OR “Meia Idade” OR “Mediana Edad”) AND
(“Palliative Care” OR “Palliative Treatment” OR “Palliative Treatments” OR “Palliative
Therapy” OR “Palliative Supportive Care” OR “Palliative Surgery” OR “Palliative Medicine”
OR “Hospice and Palliative Care Nursing” OR “Palliative Nursing” OR “Palliative Care
Nursing” OR “Hospice Nursing” OR “Hospice Care” OR “Hospice Programs” OR “Hospice
Program” OR “Bereavement Care” OR “Terminal Care” OR “End of Life Care” OR “End of
Life Cares” OR hospices OR hospice OR “Critical Illness” OR “Critical Illnesses” OR
“Critically Ill” OR “Cuidados Paliativos” OR “Assistência Paliativa” OR “Cuidado Paliativo”
OR “Tratamento Paliativo” OR “Apoyo en Cuidados Paliativos” OR “Asistencia Paliativa
de Apoyo” OR “Atención Paliativa” OR “Tratamiento Paliativo” OR “Medicina Paliativa”
OR “Enfermagem de Cuidados Paliativos na
|
1
|
The search was conducted in the following databases: Medline/ PubMed (Medical Literature
Analysis and Retrieval System Online); BVS/Lilacs (Latin American and Caribbean Health
Sciences Literature); Embase (Excerpta Medica dataBASE); Scopus; Cinahl (Cumulative
Index to Nursing and Allied Health Literature); and Web of Science, searching for
scientific works that had covered the themes in the aforementioned PCC strategy. The
search for gray literature included a focused search in the ProQuest Dissertations
and Theses Global (ProQuest) and Google Scholar databases. From the latter, the first
199 results were included.
After exploration, the results were then selected and refined, based on the instrument
previously validated in Ursi's studies 26, which covers the following items: identification of the original article, the study's
methodological characteristics, assessment of methodological rigor, interventions
measured, and results found.
The inclusion criteria were studies that covered at least three of the four thematic
categories (nursing care + PC + the elderly + surgery), that were primary research,
systematic reviews, meta-analyses, and clinical trials, without time limits or language
limitations to provide a more comprehensive overview of the theme.
Books, documents, informative texts, editorial articles, and clinical manuals were
excluded, as well as works with restricted access or which failed to reference PC
and the perioperative environment (clinic/surgical ICU). To read the content, paid
access to the Sistema de Comunidade Acadêmica Federada da Coordenação de Aperfeiçoamento do Pessoal
de Nível Superior (Federated Academic Community System of the Coordination for the Improvement of Higher
Education Personnel) at the Universidade Federal da Paraíba was required.
The selection was based on three steps, namely: 1st step: listing the databases and
applying a pilot test to the form in the Medline database with the application of
the inclusion criteria used. 2nd step: a broad search, the exclusion of duplicate
results, title, and abstract reading to fit the PCC strategy by two independent reviewers
and a decision-maker reviewer, thus selecting the eligible materials. 3rd step: complete
reading of the eligible materials and their references.
Finally, there is no conflict of interest in this research. The study protocol is
registered on the Open Science Framework platform under DOI 10.17605/OSF.IO/HSC75.
The project was approved by the Research Ethics Committee of the Health Sciences Center
of the Universidade Federal da Paraíba, Brazil, under ethics review certificate 67165623.0.0000.5188. The ethical requirements
complied with the norms governed by Resolutions 466/2012 and 510/2016 of the Brazilian
Ministry of Health.
Results
In the present review, 509 studies were found, distributed as follows: 142 (27.89
%) found in PubMed/Medline; 136 (26.71 %,) in Embase; 80 studies (15,71 %) in Scopus;
CINAHL with 61 (11.9 %); Web of Science with 26 (5.10 %), and Lilacs with one study
(0,19 %). The gray literature repositories represented 202 productions (39.68 %) in
the sample, of which three were from ProQuest Dissertations (0.58 %) and 199 from
Google Scholar (39.09 %). In addition, 22 (4.32 %) publications were included when
reading references and citations found on the websites and repositories of autonomous
organizations.
After applying the PCC strategy and refining it, the final sample consisted of 13
articles (2.55 % of the total), which were published between 2001 and 2023 (22 years).
All these works were scientific articles published in journals. Table 2 presents the reference data, objectives, method, population, findings, and considerations
of the studies regarding the technologies and strategies used for the palliative treatment
of elderly surgical patients.
Table 2
Characteristics of the Studies of the Scoping Review Sample
|
|
Article title/authors
|
Country/ year
|
Journal
|
Study design
|
Participants
|
Objective
|
Important results
|
|
1
|
The Geriatrics Surgery Verification Program and the Life-Sustaining Treatment Decisions
Initiative: Coupling Two Programs to Improve Advanced Care Planning for Older Veterans
Undergoing Surgery/ Unruh MJ, Jones TS, Horney C, Davidson S
|
USA/2023
|
Journal of Pain and Symptom Management
|
Retrospective cohort, data collection from electronic medical records
|
N = 1264 veterans aged 65 and over
|
To evaluate the effectiveness of combining war veterans’ programs to improve advanced
care planning for the elderly undergoing surgery.
|
The percentage of veterans who completed an advanced directive increased from 38 %
to 78 %.
The study also found that the percentage of veterans who discussed their end-of-life
care preferences with their providers increased from 53 % to 88 %.
There is a need to ensure that elderly people undergoing surgery have the opportunity
to discuss their preferences with their providers and make informed decisions about
their care.
|
|
2
|
Palliative Care Interventions for Surgical Patients: A Systematic Review/ Lilley EJ,
Khan KT, Johnston FM, Berlin A, Bader AM, Mosenthal AC, Cooper Z
|
USA/2021
|
JAMA Surgery
|
Systematic review
|
N = 8575 single patients in the 25 articles analyzed
|
To evaluate the effect of PC interventions on surgical patients.
|
The study focused on establishing preoperative interventions for decision- making,
improving the quality of communication, symptom management, and reducing the use of
healthcare resources to lower costs.
PC interventions can be an important part of surgical patient care.
|
|
3
|
The Quality of Palliative Care from the Perspectives of the Elderly with Cancer at
Firoozgar Hospital in 2019: A Cross-sectional Study/ Farzadnia F, Bastani F, Haghani
H
|
Iran/2021
|
Iran Journal of Nursing
|
Quantitative descriptive study
|
N = 200 elderly cancer patients
|
To evaluate the quality of PC from the perspective of elderly cancer patients admitted
to surgical/ clinical wards.
|
Pain management and psychological support, according to the study, were insufhcient,
reducing the quality of dying in Iran.
The findings of this study can be used to improve the quality of PC for elderly cancer
patients.
The researchers recommend developing a specific structure for nurses to provide PC
to cancer patients.
|
|
4
|
The Role of the Advanced Practice Nurse in Geriatric Oncology Care/ Morgan B, Tarbi
E
|
USA/2019
|
Seminars in oncology nursing
|
Literature review
|
Number of participants not stated
|
To evaluate the role of advanced practice nurses in geriatric oncology care.
|
Nurses should formulate a care plan, provide psychosocial support to the family, and
promote dehospitalization in PC.
Addressing geriatric syndromes such as incontinence, delirium, pressure damage, falls,
and functional decline.
|
|
5
|
Palliative Nursing Care as Applied to Geriatric: An Integrative Literature Review/
Guerrero JG
|
USA/2019
|
Nursing Palliative Care
|
Literature review
|
Number of participants not stated
|
To evaluate the role of nurses in providing PC for the elderly.
|
The actions found in the study were evaluation of physical symptoms such as pain,
dyspnea, fatigue, and nausea, providing emotional and psychological support, coordinating
care and education, and participating in ethical discussions.
The nursing team is essential in ensuring that the elderly receive the care they need
to enjoy quality of life at the end of life.
|
|
6
|
Perioperative Palliative Care Considerations for Surgical Oncology Nurses/Sipples
R, Taylor R, Kirk-Walker D, Bagcivan G, Dionne- Odom JN, Bakitas M
|
USA/2016
|
Seminars in Oncology Nursing
|
Literature review
|
Number of participants not stated
|
To explore the opportunities for incorporating PC into the management of perioperative
oncology patients.
|
Symptom management, facilitating communication and decision making, psychosocial support,
and working on transitions and continuity of care are the actions listed by the study
concerning nursing professionals.
The article highlights the need for formal education in PC and the resources available
to surgical oncology nurses.
|
|
7
|
Comfort in Palliative Care: The Know-How of Nurses in General Hospital/Durante ALTC,
Tonini T, Armini LR
|
Brazil/2014
|
Journal of Nursing UFPE/ Revista de Enfermagem UFPE
|
Qualitative descriptive study
|
N = 30 nurses working in medical- surgical clinics
|
To identify nursing care related to the comfort of patients undergoing PC.
|
The nurses in the study prioritize interventions to promote comfort, including pain
management, symptom management, dyspnea, hygiene, and oxygen therapy.
They also request support from the multi- professional team and, finally, provide
emotional and spiritual support.
There is a recommendation for these professionals to prioritize the development of
a care plan, improve communication, and for hospitals to develop and implement policies
and procedures that support the provision of comfort care.
|
|
8
|
When the end is near: An ICU patient who died at home/de Vries AJ, van Wijlick EHJ,
Blom JM, Meijer I, Zijlstra JG
|
Netherlands /2011
|
Nederlands Tijdschrift Voor Geneeskunde
|
Experience report
|
A 64-year-old elderly person N = 1 participant
|
To describe the process of transferring a 64-year-old surgical patient from an ICU
to their home.
|
The transfer of care, the role of the nursing team, the following administrative steps,
the natural cause of death as a requirement factor in PC, and dehospitalization.
Nursing actions included pain and dyspnea management, oxygen therapy, continuous monitoring,
psychological and emotional support, support for patient transportation, and assistance
for a peaceful death.
|
|
9
|
The cardiovascular intensive care unit nurse’s experience with end-of-life care: A
qualitative descriptive study/Calvin AO, Lind CM, Clingon SL
|
USA/2009
|
Intensive & critical care nursing
|
Qualitative descriptive study
|
Surgical ICU nurses. N = 19 participants
|
To understand ICU nurses’ perceptions of their roles and responsibilities in end-of-life
care.
|
Nurses feel they are “walking a thin line” between providing comfort and prolonging
life, with a sense of moral distress when they are unable to provide comprehensive
care. There is pressure from medical doctors to continue interventional treatment,
even when it is clear the patient is dying.
Nurses need more support to manage the emotional and psychological demands of providing
end-of-life care, such as training, counseling, and other services.
|
|
10
|
Palliative care needs of patients with neurologic or neurosurgical conditions/Chahine
LM, Malik B, Davis M
|
USA/2008
|
European Journal of Neurology
|
Retrospective review of medical records
|
Elderly people aged 70 on average. N = 177 participant cases
|
To examine the CP needs of elderly patients with neurological and neurosurgical conditions.
|
The establishment of comfort measures, including the start of morphine administration,
the identification of candidates for PC, and the establishment of advance directives.
Patients with neurosurgical conditions have a high prevalence of symptoms such as
dysphagia, pain, dyspnea, generalized weakness, and dysarthria.
|
|
11
|
Weaning readiness and fluid balance in older critically ill surgical patients/Epstein
CD, Peerless JR
|
USA/2006
|
American Journal of Critical Care
|
Prospective cohort
|
Elderly people aged from 60 to 87 N = 40 participants
|
To develop a clinical profile of elderly patients successfully discharged from prolonged
mechanical ventilation.
|
Critically ill patients undergoing surgery can be discharged from ventilator use and
PC can guide the process through their principles of symptomatic management.
Performing fluid balance, in addition to examining and supporting patients and their
families, are the main nursing actions.
|
|
12
|
Palliative care in the surgical ICU/Mosenthal AC
|
USA/2005
|
Critical Care Medicine
|
Literature review
|
Number of participants not stated
|
To raise awareness of the importance of PC in surgical ICUs.
|
The administration of opioids, assistance in the preparation of PC protocols, attention
to the routes of medication administration, reducing the number of routine nursing
procedures as far as possible, e.g., turning, suctioning, manipulation of intravenous
catheters, blood collection, and checking vital signs frequently, are all actions
mentioned in the study.
Healthcare professionals should receive training and education on PC so they can provide
the best possible care to their patients.
|
|
13
|
Nursing older dying patients: Findings from an ethnographic study of death and dying
in elderly care wards/ Costello J
|
USA/2001
|
Journal of Advanced Nursing
|
Ethnographic research
|
N = 74 elderly patients N = 29 nurses N = 8 medical doctors
|
To explore the experience of terminally ill patients and nurses working with elderly
patients in the management of end-of-life care.
|
Terminal care for some elderly patients remains hampered by the reluctance of nurses
and medical doctors to be more open in their communication about death.
Hospital culture and the customs, beliefs, and ideologies that emanate from the biomedical
model significantly shape the experiences of terminally ill elderly patients.
|
Of the 13 articles selected, in terms of methodological design, most were exploratory
quantitative or qualitative studies (30.76 %) and literature reviews -either systematic
or integrative (38.46 %). Regarding where the research was conducted, most studies
were from the USA, with a total of 10 (76.92 %).
The total population of this scoping review, considering all the studies included,
totaled 10,417 people, consisting of 10,331 unique patients, 78 nurses, and eight
medical doctors. The patients' ages ranged from 60 years to a maximum of 109 years
(study 10).
The nursing interventions cited the most in the articles were, in the first place,
the establishment of physical comfort measures, such as symptom management and the
administration of opioids, as well as the reduction of care activities considered
unnecessary, with seven (53.84 %) studies addressing these topics. Seven publications
(53.84 %) also cited the need for communication and biopsychospiritual support from
nurses toward patients and their families, highlighting the importance of this item
for care.
A total of three (23.07 %) studies addressed the ethical dilemmas of PC, such as nurses
facing moral anguish due to the impasse between recognizing the imminence of death
and following medical protocols. Or dilemmas such as nurses' inability to empathize
with palliative patients, failing to reach a position of support and understanding.
Three other studies (23.07 %) addressed points such as the need to establish operational
protocols for better management of procedures and the nursing team's need for training
in PC. Two articles discussed the establishment of advance directives of will, the
establishment of a chain of care transfer as a means of dehospitalizing palliative
elderly individuals, referring them to hospices or to their own homes.
Lastly, a set of five (38.45 %) studies individually addressed other topics related
to the theme, such as patient eligibility, the issue regarding the costs incurred
in a situation of clinical mismanagement, the proposal of a preoperative structure
with nursing appointments, a protocol for early ventilator discharge, and care for
an adequate end-of-life situation.
Figure 2 presents the frequency and grouping of the most recurrent keywords in the 13 studies.
The studies were fully imported into the VOS viewer software, analyzed bibliometrically,
and grouped by similarity, trend, recurrence, and time in the form of networks. The
groups highlighted refer to dysthanasia, the causes that lead patients to PC and,
lastly, palliative nursing actions and interventions.
Figure 2
Bibliometric Frequency, Recurrence, and Temporal Grouping of Keywords Dysthnasia
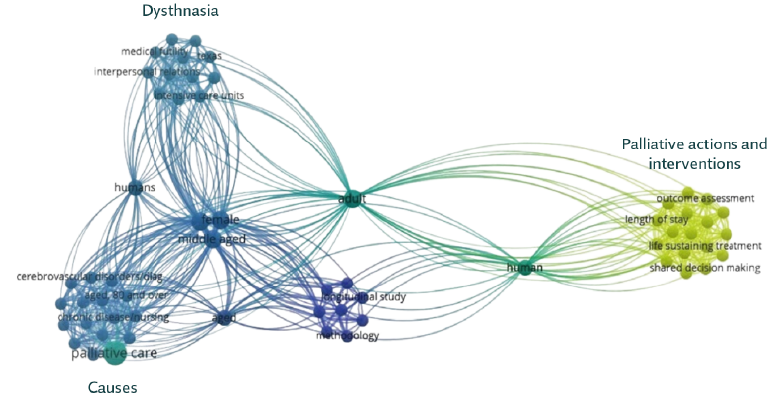
Source: Elaborated by the authors.
Discussion
Regardless of the fact that the discussion on PC dates back to the 1960s, it is essential
to highlight its relevance as a basic, structuring, and humanizing guideline for end-of-life
care, as well as to emphasize that it will take a long time for it to be fully implemented
in a surgical setting 1,27-29.
Therefore, from the analysis of this review's results, it is clear that some points
central to PC need to be promoted when compared to overpowering variables, such as
population aging and the number of people living with progressive chronic diseases
with no prospect of a cure.
First of all, it is necessary to consider the inequality in access to this type of
care and its reach in population terms, which has occurred mostly in the planet's
most developed regions. This review's results show this disparity based on the volume
of scientific production stemming from North America and Europe, a fact corroborated
by Andrade et al. 30, who state that most of the high-evidence studies come from the USA, Canada, and
the United Kingdom, which are wealthier and have a wider reach in terms of palliative
care 16.
In this sense, the scope of care in demographic terms is clearly difficult in less
developed regions. In the USA, for instance, 20,000 of the world's 100,000 palliative
care services exist, with an increase of 267 % in 20 years (from 1985 to 2005 [1,
2, 31, 32]). In Latin America, 1562 palliative care services currently exist for a
demand of approximately 12 million people who need this type of care 33,34. However, only 10 % of these people have access to this type of care, i.e. 2.6 services
for every million inhabitants 2,16.
In Brazil, this ratio is of just 0.96 teams per million inhabitants, and according
to the European Palliative Care Association, 20 services per million people are recommended
16,33. Although incipient, this scenario does not necessarily mean that PC will no longer
be provided. However, situations involving coping with death would be better handled
in the presence of specialized teams. In addition, suppressed demand, social inequalities
in health, and limited access to opioids and palliative services mean that the quality
of death in the country is considered poor. In a ranking of the quality of death in
81 countries, Brazil ranked 41st, behind neighboring countries such as Chile (27th),
Argentina (32nd), and Uruguay (37th [35]).
With that said, the first point to note from this review's results is the management
of physical symptoms and pain, which is vital to the quality of end-of-life care.
Pain management is the most relevant topic when it comes to minimizing the suffering
of PC patients and, in this regard, the availability of analgesic medication is inadequate
in Brazil and most parts of the world due to concerns regarding illicit use and drug
trafficking 36-38.
In the symptomatic context, which also includes dyspnea, nausea, delirium, and fatigue,
nurses must make adequate assessments and use their knowledge to responsibly administer
medication such as opioids, which are the basis of analgesic treatment in palliation
(36, 39). Studies 40,41 show that in the administration of opioids, such as morphine, codeine, and fentanyl,
the presentations and administration routes are factors that trigger doubts in nurses,
who have this deficiency at the heart of their training. Kulkamp, Barbosa, and Binchini
42 state that myths such as the uncertainty of dosage, fear of addiction, tolerance
and/or side effects of opioids often lead nurses to be reluctant to administer them.
It should be noted that poorly managed pain generates costs, is debilitating, and
terrorizes patients and their families, affecting their physical, emotional, and spiritual
well-being. The American Pain Society and the National Comprehensive Cancer Network
found that nurses had low or moderate knowledge in a survey on pain management, which
shows that their knowledge in varying contexts is still deficient and needs to be
improved 43.
Recently, studies on the use of alternative therapies for symptomatic management have
proven promising 44,45. As it is a multidimensional phenomenon, pain deserves to be addressed from various
perspectives and with a multi-professional approach. Acupuncture, acupressure, reflexotherapy,
logotherapy, and phytotherapy are the main alternative therapies used, with special
emphasis on the use of cannabinoid derivatives, which have been efficiently reported
in recent studies with anti-emetic, neuroprotective, anti-inflammatory, and anti-cancer
properties, and may be beneficial in the palliative treatment of perioperative cancer
pain and psychic disorders 46.
Another key dimension of discussion according to the research results is the cultural
one, namely the permeability of PC in the surgical setting, especially in terms of
patient eligibility and the early start of the palliative approach. The growing complexity
of critically ill surgical patients creates an ideal opportunity for early integration
into continuous care 47.
Thus, it is worth mentioning Bonnano's study 48, which compared the care provided in the traditional model and in the early PC model,
in which the group that received palliative care had better self-assessments of quality
of life and lower scores on scales measuring mood disorders. In addition, these patients
lived on average three months longer than the group that received care in the traditional
model and, as a result, plenty has been studied and it is increasingly proven that
early palliative care has a positive impact on patients' lives 48.
One intervention cited in the results is the study by Walling et al. 49, which simulates a clinic model incorporated into preoperative care, in which a trained
nursing professional provides specialized outpatient care, immediately prior to the
medical consultant, allowing direct referrals and assistance focused on end-of-life
care. This model is currently used in several US oncology clinics and is growing in
other specialties, notably in cardiology and surgical oncology.
Other interventions that could benefit patients in preoperative care are those aimed
at characterizing the patient's profile, their possible eligibility for PC, the creation
of a personalized care plan, and the establishment of advance directives to provide
an additional level of perioperative palliative care.
In the meantime, the nursing field needs to work on dissociating itself from a purely
technical and prescriptive care practice towards an emphasis on the person, on solidarity,
on optimizing the quality of life by discussing each patient's general care objectives
and thus devising a transition plan for home care and nursing homes 27,50. The findings of this review indicate that in some cases, surgical nursing procedures
-punctures, test collections, decubitus changes, invasive monitoring, ICU blood glucose
checks, and intensive care maintenance- are considered unnecessary from a palliative
point of view and could be postponed for the benefit of the client's well-being at
the time, are routine and performed unquestionably by the team 51.
A care transition plan, as mentioned above, combined with educating families and raising
awareness of actions in line with the patient's needs and wishes, promotes these elderly
people's de-hospitalization when possible, significantly improving their quality of
life and their perception of the end of life. Dyar 52 corroborates the above by stating that, despite all the efforts involved, the quality
of dying in a hospital remains poor and, in this regard, the transfer of care and
de-hospitalization provide quality and a new meaning to the end of life.
These simple perspectives can make a significant difference. Diverging from a curative,
bio-technical, and disease-focused conception is crucial to generate subsidies that
provide the best way to live in terminality when one is in the shadow of a reserved
diagnosis. In this context lies the colossal cultural challenge posed by the perioperative
environment, in which a strong paternalistic pressure is present 33,53.
Data from this review show the conflicts faced by nurses in their role as autonomous
providers and patient advocates versus their protocol role in technical healthcare
54. According to Elpern, Covert, and Kleinpell 55, nurses generally perceive medical doctors as the legitimate initiators of this discussion,
as well as the final decision-makers. However, in the surgical clinic setting, there
is a significant obstacle to communication and dialog with medical professionals,
who strangely persist in the misconception of reducing palliative care, resulting
in patients being isolated behind a wall of words or in silence and preventing therapeutic
adherence and the sharing of fears, anxieties, and concerns 56.
Therefore, several professional nurses find themselves in a difficult situation when
they have to follow invasive protocols despite knowing that they are inconsistent
with the patient's health condition 54. Faced with their prognostic awareness, the veiled distress of the families and the
medical position, this results in moral an guish suffered by this professional category
in their practice in palliation settings 54,55.
In the same issue, there is also the reluctance of nurses to communicate information
regarding the patient's condition, which, without correct strategies or in a purely
empirical way, leaves them in the dark concerning the diagnosis of their condition
50. Thus, another categorized dimension emerges from this review's results: that of
nurses' communication regarding elderly patients' condition in clinics and surgical
ICUs.
Some nurses find it extremely difficult to talk to patients and their families about
their condition, restricting the discussion to purely technical aspects or empirical
approaches that reproduce cultural preconceptions. According to Oliver et al. 57, the greatest aspect to overcome in terms of communication is truthfulness and an
unwillingness to engage meaningfully with patients on sensitive issues. Studies have
discussed the problems associated with providing care to dying patients and found
trivial issues related to truthfulness and unwillingness to engage meaningfully in
discussions with patients about death 55,57,58.
Nurses are generally skilled at providing care, managing physical symptoms, and controlling
the environment, as their Night-ingalean heritage is based on basic human needs, so
they provide responsible perioperative care. However, they fall short in aspects such
as emotional involvement with patients, institutionalized non-disclosure of information
about the process of death and dying, and reluctance to be more open in their communication
54,59. Despite the improvements made in the provision of individualized care for dying
patients, their care does not seem to overcome some of the most important aspects,
such as communication 59.
The applicability of PC in a surgical environment in the nursing field is also limited
for other reasons. One of them is the lack of understanding and integration into biological
scenarios. Several nurses have limited knowledge about the role of PC in surgery,
which results in late or inadequate provision to patients in this condition 60.
Therefore, it is necessary to train these professionals in PC through education programs
aimed at providing collaboration, so that they can work collaboratively with the surgical
team, ensuring holistic care for surgical patients and facilitating effective communication
and decision-making 60. In addition, it is necessary to provide ethical decision-making training to them,
with frameworks and principles to address dilemmas to balance patient autonomy, beneficence,
and non-maleficence 47. Finally, training in communication skills is also needed, including how to handle
bad news, discuss treatment options, and facilitate end-of-life directives. These
are implementations that can increase their ability to communicate sensitively and
empathetically with patients and their families.
Finally, the process of synthesizing this review's findings was relatively hindered
by the scarce evidence on interventions to introduce or improve PC in surgical patients,
in addition to being limited by methodological approaches, in which rigorous and standardized
evaluations are needed that also measure significant results for patients. However,
all the studies presented results that satisfy the proposed practice and contribute
to its implementation.
The models aim to integrate perioperative approaches and reiterate the need to rethink
healthcare in an attempt to foster more socially connected, planned, and person-centered
care.
Conclusions
It is known that elderly people with serious illnesses with surgical referrals can
benefit from a specialized approach to PC in the perioperative setting. This review
aims to describe and systematize the methods and practices used by the nursing team
to provide PC to elderly patients in a highly technical environment, with hard technologies
and a high expectation of recovery: the perioperative period.
There is a need to improve nurses' knowledge in the administration of opioids and
alternative technologies to manage pain. There is also a need to empower these professionals
to participate in ethical decisions, devise a plan aimed at transferring care, and
train them to communicate more effectively with patients and their families. Through
clear criteria and to reduce bias in the collection and selection of references, the
data compiled in this review will contribute to strengthening actions aimed at the
person, symptoms, and communication, which are commonly used in care management in
the biopsychosocial and spiritual spheres.
Notwithstanding the above, this study does not end in itself but rather sheds light
on the need for more studies aimed at understanding the needs and priorities of the
capillarization of PC as an effective practice in a surgical setting and understanding
the structural inequalities in the provision of this type of care. Thus, it constitutes
a starting point for re-signifying not only healthcare in particular but also the
dimension of care as a whole.
