
|
|
ARTICLE

Luisa Fernanda Achury-Beltrán 1
Juliette Marie Brito-Suárez 2
Judy Ximena Ramos-Garzón 3
Ángela Marcela Ramírez-Cárdenas4
1 Pontificia Universidad Javeriana, Colombia
![]() 0000-0001-6931-396X
0000-0001-6931-396X
![]() achuryl@javenana.edu.co
achuryl@javenana.edu.co
2 Universidad Nacional Autónoma de México, México
![]() 0000-0002-8388-9241
0000-0002-8388-9241
![]() juliette.brito@comunidad.unam.mx
juliette.brito@comunidad.unam.mx
3 Universidad Industrial de Santander, Colombia
![]() 0000-0002-8459-076X
0000-0002-8459-076X
![]() jxramosg@uis.edu.co
jxramosg@uis.edu.co
4 Fundación Cardioinfantil, Colombia
![]() 0000-0003-3240-6964
0000-0003-3240-6964
![]() angel_6584@hotmail.com
angel_6584@hotmail.com
Topic: Care processes and practices
Contribution to the discipline: This study contributes to the disciplinary knowledge of nursing, as it highlights the need for more comprehensive communication with the families of critically ill patients in intensive care units. By recognizing that communication activities primarily focus on the transmission of information, with less emphasis on psycho-spiritual needs, the importance of developing strategies that more comprehensively address the concerns and emotions of family members becomes evident. Ultimately, it highlights the impact of work overload on the performance of these activities, which has a direct effect on the quality of the care provided.
Received: 14/07/2024
Sent to peers: 19/09/2024
Approved by peers: 14/04/2025
Accepted: 29/04/2025
To reference this article / Para citar este artículo / Para citar este artigo Achury-Beltrán LF, Brito-Suárez JM, Ramos-Garzón JX, Ramírez-Cárdenas ÁM. Nursing Professionals’ Perceptions of Communication with the Family of a Critically Ill Patient -Colombia. Aquichan. 2025;25(3):e2533. DOI: https://doi.org/10.5294/aqui.2025.25.3.3
Abstract
Introduction: Communication between nursing professionals and the families of critically ill patients is an essential aspect of quality care. Therefore, measuring this communication is an important factor in improving healthcare. The objective was to determine the communication activities performed by nursing professionals with the families of critically ill patients and their association with sociodemographic variables.
Materials and Methods: This was an analytical cross-sectional study with a purposeful sample of 100 intensive care nursing professionals from the Colombian Andean Region. The instrument Nursing Activities to Communicate with the Families of Critically Ill Patients was used, which consists of 16 items and has an overall Cronbach's alpha of 0.92. Descriptive statistics and bivariate analysis were applied; the significance level was set at 0.05.
Results: Nursing professionals "almost always" develop communication activities aimed at transmitting information and "sometimes" activities focused on identifying and satisfying psycho-spiritual needs. The variables most associated with communication activities were the number of patients assigned and the educational level (p < 0.05).
Conclusions: Information is a priority for the families of critically ill patients, so communication activities related to physical, emotional, cultural, and relational aspects are essential in nursing care. However, some variables can limit communication. Communication activities by nursing professionals should be strengthened to enhance the quality of care provided to the families of critically ill patients.
Keywords (Source: DeCS): Family nursing; critical care; communication; family; professional-family relationships
Resumen
Introducción: La comunicación entre el profesional de enfermería y la familia del paciente crítico es un aspecto imprescindible en la calidad del cuidado, por lo tanto, su medición es un insumo relevante para mejorar la atención en salud. El objetivo fue determinar las actividades de comunicación desarrolladas por el profesional de enfermería con la familia del paciente crítico y su asociación con las variables sociodemográficas.
Materiales y método: Estudio transversal analítico, con una muestra intencional de 100 profesionales de enfermería de cuidado intensivo de la Región Andina colombiana. Se usó el instrumento "Actividades de enfermería para comunicarse con las familias de pacientes críticos", el cual cuenta con 16 ítems y un alfa de Cronbach global de 0,92. Se aplicó estadística descriptiva y un análisis bivariado; el nivel de significación se fijó en 0,05.
Resultados: Los profesionales de enfermería desarrollan "casi siempre" actividades de comunicación dirigidas a la trasmisión de información y "algunas veces" actividades centradas en la identificación y satisfacción de necesidades psicoespirituales. Las variables más asociadas con las actividades de comunicación fueron el número de pacientes asignados y el nivel de estudios (p < 0,05).
Conclusiones: La información es una necesidad prioritaria para los familiares de pacientes críticos, por lo que actividades de comunicación relacionadas con aspectos físicos, emocionales, culturales y relacionales son esenciales en el cuidado de enfermería. No obstante, algunas variables pueden limitar la comunicación. Deben fortalecerse las actividades de comunicación por parte del profesional de enfermería, de manera que se mejore la calidad de cuidado brindado a la familia del paciente crítico.
Palabras clave (Fuente DeCS): Enfermería de la familia; cuidados críticos; comunicación; familia; relaciones profesional-familia
Resumo
Introdução: A comunicação entre o profissional de enfermagem e a família do paciente crítico é um aspecto essencial na qualidade da assistência. Sua mensuração constitui, portanto, um insumo relevante para a melhoria da atenção à saúde. O objetivo foi determinar as atividades de comunicação desenvolvidas pelo profissional de enfermagem com a família do paciente crítico e sua associação com variáveis sociodemográficas.
Materiais e método: Estudo transversal analítico, com amostra intencional de 100 profissionais de enfermagem de unidades de terapia intensiva da Região Andina colombiana. Utilizou-se o instrumento "Atividades de enfermagem para a comunicação com familiares de pacientes críticos", composto por 16 itens e com alfa de Cronbach global de 0,92. Foram aplicadas estatísticas descritivas e análise bivariada; o nível de significância adotado foi de 0,05.
Resultados: Os profissionais de enfermagem realizam "quase sempre" atividades de comunicação voltadas à transmissão de informações e "às vezes" atividades centradas na identificação e satisfação de necessidades psicoespirituais. As variáveis mais associadas às atividades de comunicação foram o número de pacientes sob responsabilidade do profissional e seu nível de escolaridade (p < 0,05).
Conclusões: A informação é uma necessidade prioritária para familiares de pacientes críticos; portanto, atividades de comunicação relacionadas a aspectos físicos, emocionais, culturais e relacionais são essenciais na assistência de enfermagem. No entanto, algumas variáveis podem limitar a comunicação. As atividades de comunicação do profissional de enfermagem devem ser fortalecidas, a fim de melhorar a qualidade da assistência prestada à família do paciente crítico.
Palavras-chave (Fonte DeCS): Enfermagem da família; cuidados intensivos; comunicação; família; relações profissional-familiar
Introduction
Over the last few decades, critical patient care, family-centered care, and the trend toward humanization in intensive care units (ICUs) have made increasingly clear how important families are, not only as a key resource in patient recovery by offering a potential opportunity for collaboration in the ICU and acting as facilitators in shared decision-making 1, but also as a focus of nursing care 2.
Despite this context, in practice, it is perceived that within ICUs, greater importance is given to the care of critical patients, largely ignoring the fact that the family perceives the experience as a catastrophic situation 3. To our knowledge, in the Colombian context, there is insufficient evidence of communication activities that allow the families of critical patients to be recognized as subjects of care with specific needs.
Some research has found that adequate information and communication are the priority needs of families of critically ill patients 4,5, as they ensure the provision of consistent, realistic, and timely data on the patient's health and the effectiveness of the treatments implemented, as well as honest answers about the prognosis and acceptance of the situation.
Within the framework of nursing references, interpersonal relationship theories support the therapeutic bond that is created between the patient and the nursing professional. An example of this is Hildegard Peplau's proposal, whose theory focuses on the phenomenon of the person-to-person relationship, through which a meaningful interpersonal process is generated that allows for the satisfaction of needs 6. On the other hand, in Imogene King's theory, which focuses on the interpersonal system, the nurse-patient relationship has as its central component the communication of information, which facilitates the achievement of joint objectives and goals. King defines communication as any behavior that expresses objectives and values and that can occur from one person to another, either face-to-face or indirectly through different channels 6.
In this way, communication becomes an essential aspect of care, as it increases family satisfaction 7, trust in healthcare personnel, and the psychological well-being of family members, in addition to strengthening the empathetic relationship between the nursing professional and the family 8. All these aspects, based on Jean Watson's proposal for humanized care, are linked to empathy and active listening, directly connecting with the communication processes that nurture the therapeutic bond 6.
The Joint Commission International 10 has identified effective communication as a quality standard, enabling optimal patient care outcomes, reducing risks, and improving health outcomes. However, some authors 4 consider that family members do not receive sufficient guidance on the patient's situation in the ICU context, nor adequate guidelines for interacting, which, added to the breakdown of the patient-family unit and the potential lack of communication with healthcare staff, constitutes an environment that can generate disturbing situations, interpersonal conflicts, and a negative impact on the quality of care perceived by the family 10.
Communication and the establishment of appropriate channels are fundamental in recognizing and meeting the needs of the critically ill patient's family. In this way, establishing the activities that nursing professionals perform to communicate with the family in the national context allows them to identify the strengths and aspects that need to be reinforced in the care process and, with this, highlight options for improvement that refine the process of caring for the family in the hospital setting.
Therefore, the primary objective of this study was to describe the communication activities that nursing professionals develop with the families of critically ill patients in the Colombian context.
Methodology
Design and Scope
A cross-sectional analytical study was conducted to evaluate the communication activities that nursing professionals performed with the families of critically ill patients in the Colombian Andean Region between December 2020 and December 2021. The STROBE guidelines for observational studies were followed.
Subjects
The population consisted of nursing professionals who worked in various adult ICUs and had at least six months of experience in the field. No exclusion criteria were considered, other than failure to complete the entire survey. A consecutive non-probability sampling method was used until a sample of 100 participants was completed.
Variables
Sociodemographic data such as age, gender, marital status, working hours, number of patients assigned, highest educational level, and type of unit where they work were collected. The main variable was the communication developed by the nursing professional with the family of the critically ill patient, which was measured in the development of activities.
Procedure
The instrument Nursing Activities for Communicating with Families of Critically Ill Patients, developed by Curtis et al. 11, was used. It consists of 16 items scored on a Likert scale and has a Cronbach's alpha of 0.88 in its English version 12. It was translated in Spain by Santana et al. 13, and its validated and adapted version for the Colombian population reported an overall Cronbach's alpha of 0.92 14. Permission to use the instrument was obtained from its authors.
Nursing professionals were contacted electronically and invited to complete the available online instrument after accepting participation in the research through an electronic consent. The results were migrated to an Excel matrix, which was reviewed and refined for final analysis, performed using Stata statistical software version 14 (Stata Corp, College Station, Tex, USA).
Data Analysis
Quantitative variables are presented as median and interquartile range (IQR), according to their distribution, and qualitative variables are presented in absolute and relative frequencies. In the bivariate analysis, the Kruskal-Wallis test was used for quantitative variables and Fisher's exact test for qualitative variables; the significance level was set at 0.05.
Ethical considerations
The regulations in force of the Council of Medical Science Organizations, the WHO, and Resolution 008430 of 1993 of the then Ministry of Health of the Republic of Colombia were considered. Nursing professionals participated voluntarily and approved their participation in the research, accepting an electronic informed consent form. The confidentiality of the information was maintained by assigning each participant a consecutive number; the information is stored on the principal investigator's computer. The research project was approved by the Research and Ethics Committee of the Faculty of Nursing at the Pontificia Universidad Javeriana (Minutes 004 of September 3, 2018).
Results
The participants were mostly women, single, with a median age of 34, located geographically in the Andean Region, with the highest level of specialized education and a median of 7 years of work experience in ICUs, belonging to medical units, and working rotating shifts, as shown in Table 1.
Table 1 Sociodemographic Characteristics of Participants
Variable |
n (%) |
|
|---|---|---|
Age (years) (Median, IQR) |
34 (29.5-38) |
|
Sex |
Female |
78 (78) |
Male |
22 (22) |
|
Marital status |
Married |
26 (26) |
Single |
49 (49) |
|
Divorced |
3 (3) |
|
Free union |
21 (21) |
|
Widower |
1 (1) |
|
Educational level |
University diploma |
4 (4) |
University |
25 (25) |
|
Specialization |
57 (57) |
|
Master's degree |
14 (14) |
|
Experience in Intensive Care (years) (Median, IQR) |
6.5 (3. 11) |
|
Unit type |
Cardiovascular |
34 (34) |
Medical |
53 (53) |
|
Surgical |
13 (13) |
|
Shift |
Morning |
27 (27) |
Afternoon |
16 (16) |
|
Evening |
23 (23) |
|
Rotating |
34 (34) |
|
Number of patients assigned (Median, IQR) |
5 (4, 7) |
|
Source: Prepared by the authors.
Among the communication activities performed by nursing professionals with the families of critically ill patients, it was evident that the most developed were those in which communication was considered a tool for informing families about the illness, treatments, devices, and care plans. However, those in which communication is oriented toward identifying spiritual, cultural, and religious needs were peformed only a few times, as were those that allow the identification of the patient's wishes and acceptance of treatments, as shown in Table 2.
Table 2 Communication Activities with the Family of Critically Ill Patients
Item |
Never n (%) |
Sometimes n (%) |
Almost always n (%) |
Always n (%) |
|---|---|---|---|---|
1. Do you explain the treatment the patient is receiving to their family members? |
2 (2) |
27 (27) |
47 (47) |
24 (24) |
2. Do you explain to the family members the purpose of the devices and equipment the patient is connected to? |
0 |
23 (23) |
41 (41) |
36 (36) |
3. Do you provide the family with information about the purpose of the various care activities that are performed? |
3 (3) |
16 (16) |
49 (49) |
32 (32) |
4. Do you provide the family with information about the purpose of any meetings they may have with other members of the healthcare team? |
3 (3) |
28 (28) |
43 (43) |
26 (26) |
5. Does he/she talk to his family about his/her possible spiritual needs (finding meaning in the situation) or religious needs (relationship with a supreme being)? |
10 (10) |
46 (46) |
26 (26) |
18 (18) |
6. Do you help family members to ensure that their spiritual and religious needs are met? |
8 (8) |
35 (35) |
35 (35) |
22 (22) |
7. Do you talk to family members about their cultural needs (those of a material or ideological nature that represent a person as part of a group)? |
14 (14) |
55 (55) |
26 (26) |
5 (5) |
8. Do you help in any way to ensure that the family's cultural needs are met? |
7 (7) |
46 (46) |
33 (33) |
14 (14) |
9. Do you discuss with the family members what the patient values most in life? |
18 (18) |
40 (40) |
31 (31) |
18 (18) |
10. Do you talk to the family members about the patient's illness and the treatment he or she is receiving? |
1 (1) |
23 (23) |
38 (38) |
38 (38) |
11. Do you discuss with the family the feelings they are experiencing? |
5 (5) |
37 (37) |
36 (36) |
22 (22) |
12. Do you ask the family members if they find it difficult to talk to or touch the patient? |
14 (14) |
33 (33) |
33 (33) |
20 (20) |
13. Do you discuss with the family members what the patient would have wanted if he or she were able to participate in decision-making and accept the tests and treatments being administered? |
13 (13) |
39 (39) |
29 (29) |
19 (19) |
14. Do you inquire whether there is any disagreement among family members regarding the treatments? |
15 (15) |
45 (45) |
24 (24) |
16 (16) |
15. Do you communicate changes in the care plan to family members? |
2 (2) |
28 (28) |
43 (43) |
27 (27) |
16. Do you assure the family members that the patient is comfortable? |
1 (1) |
13 (13) |
38 (38) |
48 (48) |
Source: Prepared by the authors.
About the bivariate analysis in Table 3, the sociodemographic variables number of patients assigned, highest educational level, age, shift, and years of experience in the ICU showed an association with some of the items in the instrument (p<0.05). The items in the instrument that showed the strongest associations were "Do you discuss with the family members what the patient values most in life?", Do you inquire whether there is any disagreement among family members regarding the treatments?", and "¿Do you assure the family members that the patient is comfortable?".
Table 3 Association between Sociodemographic Characteristics and Communication Activities Performed by Nursing Professionals with the Families of Critically Ill Patients
Item |
Number off |
Age |
Years of experience |
Educational |
Shift |
|---|---|---|---|---|---|
1. Do you explain the treatment the patient is receiving to their family members? |
0.14 |
0.54 |
0.32 |
0.15 |
0.09 |
2. Do you explain to the family members the purpose of the devices and equipment the patient is connected to? |
0.03 |
0.61 |
0.96 |
0.48 |
0.08 |
3. Do you provide the family with information about the purpose of the various care activities that are performed? |
0.08 |
0.92 |
0.54 |
0.63 |
0.05 |
4. Do you provide the family with information about the purpose of any meetings they may have with other members of the healthcare team? |
0.22 |
0.29 |
0.51 |
0.29 |
0.46 |
5. Does he talk to his family about his possible spiritual needs (finding meaning in the situation) or religious needs (relationship with a supreme being)? |
0.65 |
0.28 |
0.16 |
0.77 |
0.11 |
6. Do you help family members to ensure that their spiritual and religious needs are met? |
0.17 |
0.94 |
0.85 |
0.10 |
0.67 |
7. Do you talk to family members about their cultural needs (those of a material or ideological nature that represent a person as part of a group)? |
0.95 |
0.43 |
0.66 |
0.20 |
0.21 |
8. Do you help in any way to ensure that the family's cultural needs are met? |
0.07 |
0.31 |
0.54 |
0.30 |
0.08 |
9. Do you discuss with the family members what the patient values most in life? |
0.02 |
0.75 |
0.36 |
0.79 |
0.00 |
10. Do you talk to the family members about the patient's illness and the treatment he or she is receiving? |
0.16 |
0.28 |
0.27 |
0.27 |
0.13 |
11. Do you discuss with the family the feelings they are experiencing? |
0.09 |
0.72 |
0.50 |
0.10 |
0.05 |
12. Do you ask the family members if they find it difficult to talk to or touch the patient? |
0.23 |
0.40 |
0.38 |
0.80 |
0.20 |
13. Do you discuss with the family members what the patient would have wanted if he or she were able to participate in decision-making and accept the tests and treatments being administered? |
0.30 |
0.87 |
0.97 |
0.83 |
0.70 |
14. Do you inquire whether there is any disagreement among family members regarding the treatments? |
0.65 |
0.00 |
0.00 |
0.51 |
0.29 |
15. Do you communicate changes in the care plan to family members? |
0.27 |
0.30 |
0.34 |
0.73 |
0.28 |
16. Do you assure the family members that the patient is comfortable? |
0.31 |
0.00 |
0.07 |
0.02 |
0.43 |
Source: Prepared by the authors. * Kruskal-Wallis Test; ** Fisher's exact test.
As shown in Figure 1, there was an inverse trend toward discussing with the family members about what the patient values most in life, with less frequency when there is a higher assignment of patients; this association was statistically significant (p<0.05).
Figure 1 Association between Item 9 and the Number of Patients Assigned
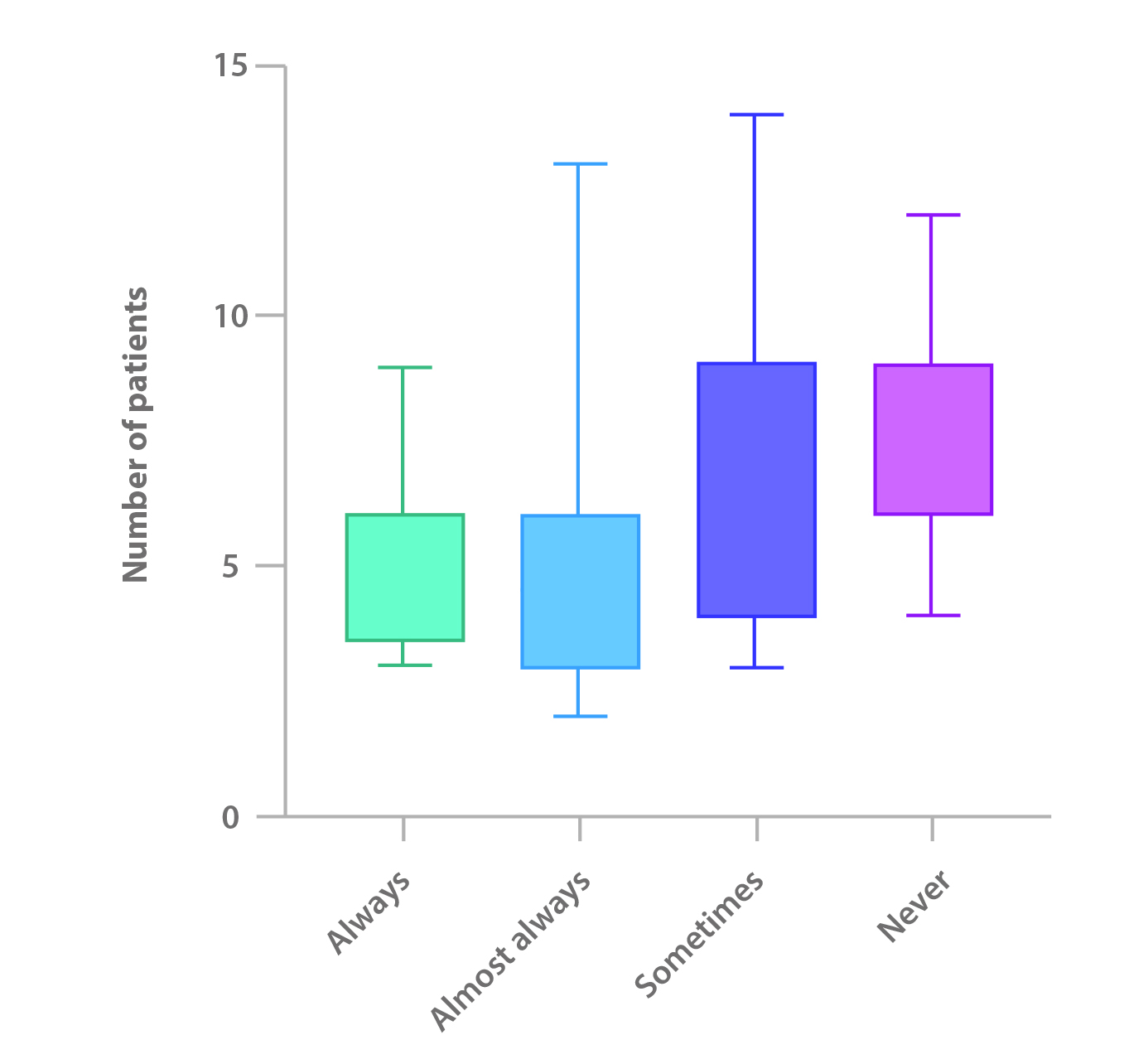
Source: Prepared by the authors.
* Kruskal-Wallis Test, p<0.05.
Discussion
The characterization of nursing professionals in our study is similar to that reported by a Latin American study 15, which shows a median age of 34 years, a predominance of females, single marital status, rotating shifts, a median ICU experience of approximately 6.5 years, and a number of assigned patients of 5 or more, which reveals the landscape of intensive care nursing professionals in the Colombian setting.
Regarding communication activities, professionals reported that they "almost always" performed them to provide information about the patient's health status, the treatments implemented, the devices installed, the purpose of the care activities performed, the objective of the meetings with other health professionals, and changes in the care plan, and to inquire about the perception of impediments to talking to or touching the patient. These data differ from other studies 13,16, where most communication activities are performed only "sometimes." Information has been described as one of the primary needs of the family of the critically ill patient 17, and therefore, the activities implemented by the professional are mostly aimed at satisfying this need and thereby reducing the harmful emotional effects associated with the situation 18. However, it is worth noting that, according to reports from professionals, some families may not receive the required information, thereby affecting their perception of the care received and generating anxiety and stress due to a lack of knowledge about the situation.
As for communication activities related to both assessment and the satisfaction of cultural, spiritual, and religious needs, these are only peformed "sometimes" by nursing professionals. This finding is similar to the reports by Cabrera and Murillo 13,16, confirming the priority given to the physical dimension of the patient in the ICU, which relegates the psycho-spiritual dimension to a secondary plane. In this context, Roze des Ordons recognizes the importance of the multidimensionality of human beings as a key element in the integrity and stability of patients and their families 18; therefore, nursing professionals must orient their actions beyond the physical context and consider, in turn, the accompaniment of a spiritual health practitioner who facilitates the adaptation process during the stay in the ICU, providing family support, building a bridge between professionals and families, facilitating difficult conversations, attending to individual needs, and promoting stress management 19.
Similar to other studies 13,16, there was little evidence of communication activities aimed at identifying the patient's wishes, the family's feelings, and agreement among family members about treatments, which may be related to the belief that these aspects are the exclusive responsibility of other health professionals. However, it should not be forgotten that nursing staff have the most contact with the family during the patient's stay in the ICU 2 and, therefore, should be more attentive to the feelings of the family members and provide emotional support through an empathetic, trusting relationship with understanding and sensitivity, which allows the impact of the ICU to be mitigated, facilitating the transition through that experience 20. Although the response "never" did not predominate in any of the communication activities, it is worth mentioning that a frequency of between 1 and 18 people per item was found, an aspect that should attract the attention of professionals in the context of recognizing the family as a subject of care in the ICU and as a key element in the patient's health recovery 2.
Likewise, the response "always" was only predominant in two of the care activities assessed by the instrument: "Do you discuss the patient's illness and treatment with his/her family members?" and "Do you reassure family members that the patient is comfortable?". These results may be influenced, on the one hand, by the importance that information related to the patient's health status has for family members and professionals 21, and on the other hand, by structural changes and changes in the functions of units in the context of the COVID-19 pandemic, where restrictions implemented to mitigate infections reduced contact between professionals and families, limiting opportunities for communication 22 and focusing conversations on the transmission of information about the patient's physical and physiological aspects, leaving other dimensions aside.
Finally, unlike Murillo's study 16, which only found an association between the type of unit and the information provided by the professional to the family about the disease and treatment, the present study found associations between communication activities and the number of patients assigned, age, years of experience in the ICU, educational level, and shift.
This study found a statistically significant difference in the association between the number of patients assigned and communication activities in which the family is informed about the devices and equipment with which the patient is equipped, and those in which the things the patient values most in life are explored. Internationally, some guidelines have been established in which the nurse-to-patient ratio should be 1:1 for ventilated patients and 1:2 in all other cases. However, in the Latin American and national context, there is no standard, which gives rise to ratios of 1:5 or more 15, an aspect that can condition the time that nursing professionals devote to interacting and communicating with the family of critically ill patients, giving greater importance to the physical dimension and relegating other family needs to the background.
The educational level of the nursing professional revealed an association with items in which communication is used by the professional to explain the treatments the patient receives, reassure family members that the patient is comfortable, and help ensure that the spiritual, religious, and cultural needs of the family are met.
Although this study did not distinguish whether postgraduate training was in intensive care, it appears that a higher educational level promotes a comprehensive view of the patient and his/ her family, strengthening the satisfaction of both physical and cultural, spiritual, and religious needs. In this sense, the study conducted by Duffield 23 found higher scores in the domains of leadership, research, education, optimization of health services, and clinical care as the level of training increased, showing a statistically significant difference in all domains except clinical care, which could partly explain the results of the present study.
This study showed a prevalence of rotating shifts, as well as an association between shifts and communication activities focused on caregiving, family feelings, and identifying the aspects that patients value most in life. Other studies also reveal a predominance of rotating shifts or shifts lasting more than one day 15,24, in which contact with the family can vary, also being associated with the established visiting policy. Some authors report that rotating shifts generate the highest workload and have the greatest impact on the health of professionals 24,25, which can affect professional performance and limit communication activities established with the families of critically ill patients. Unlike Murillo's findings 16, the present study found an association between years of work experience in the ICU and knowledge about disagreements among family members regarding treatment, which suggests that experience strengthens a comprehensive view of the human being. Edward 26 found that nurses felt very confident communicating with the families of critically ill patients, probably because 88% of the professionals had more than eleven years of experience, which confirms the importance of this variable in establishing an appropriate communication channel that has a positive impact on the family members' level of satisfaction.
Frequently, family members of critically ill patients perceive communication to be fragmented and inconsistent, leaving them dissatisfied with the communication, information shared, and emotional support received 26. This study's results highlight the urgent need for nursing professionals to strengthen their communication skills and abilities so that they can identify and meet the needs that arise during the ICU stay experience.
This research has the limitations inherent in cross-sectional studies. In addition, the professionals were geographically located in the Andean Region, so the results should not be extrapolated to the general population.
Conclusions
Nursing professionals communicate more with the families of critically ill patients to provide information about physical aspects such as the patient's illness and treatments, leaving the identification of cultural, religious, and spiritual needs in the background. The number of patients and the educational level of the nursing professionals are the variables that showed the strongest associations and, therefore, should be considered as part of nursing care planning and management to improve health outcomes for critically ill patients.
It is recommended to conduct studies with larger populations and research that assesses the effectiveness of interventions aimed at improving communication with the families of critically ill patients.
The authors declare no conflict of interest.
Referencias
1. Schwartz AC, Dunn SE, Simon HFM, Velasquez A, Garner D, Tran DQ, et al. Making Family-Centered Care for Adults in the ICU a Reality. Front Psychiatry. 2022;24;13:1-9. DOI: https://doi.org/10.3389/fpsyt.2022.837708
2. Nygaard AM, Haugdahl HS, Laholt H, Brinchmann BS, Lind R. Professionals’ narratives of interactions with patients’ families in intensive care. Nurs Ethics. 2022;29(4):885-98. DOI: https://doi.org/10.1177/09697330211050995
3. Secunda KE, Kruser JM. Patient-Centered and Family-Centered Care in the Intensive Care Unit. Vol. 43, Clinics in Chest Medicine. W.B. Saunders; 2022. p. 539-50. DOI: https://doi.org/10.1016/j.ccm.2022.05.008
4. Digby R, Manias E, Haines KJ, Orosz J, Ihle J, Bucknall TK. Family experiences and perceptions of intensive care unit care and communication during the COVID-19 pandemic. Australian Critical Care. 2023;36(3):350-60. DOI: https://doi.org/10.1016/j.aucc.2022.03.003
5. Frivold G, Ågård AS, Jensen HI, Åkerman E, Fossum M, Alfheim HB, et al. Family involvement in the intensive care unit in four Nordic countries. Nurs Crit Care. 2022;27(3):450-9. DOI: https://doi.org/10.1111/nicc.12702
6. Mastrapa YE, Gibert Lamadrid M del P. Relación enfermera-paciente: una perspectiva desde las teorías de las relaciones interpersonales. Rev. cuba. enferm. [Internet]. 2016;32(4). https://revenfermeria.sld.cu/index.php/enf/article/view/976
7. Fortunatti CP, Silva NR, Silva YP, Canales DM, Veloso GG, Acuña JE, et al. Association between psychosocial factors and satisfaction with communication in family members of intensive care unit patients during COVID-19 pandemic: An exploratory cross-sectional study. Intensive Crit Care Nurs. 2023;76. DOI: https://doi.org/10.1016/j.iccn.2023.103386
8. Duque-Ortiz C, Arias-Valencia MM. Nurse-family relationship in the intensive care unit. Towards an empathic understanding. Revista Ciencias de la Salud. 2021;19(1):1-20. DOI: https://doi.org/10.12804/revistas.urosario.edu.co/revsalud/a.10059
9. Joint Commission International. Joint Commission International Accreditation Standards for Hospitals; 2020.
10. Garcia De Cezar A, Del Castanhel F, Grosseman S. Needs of family members of patients in intensive care and their perception of medical communication. Critical Care Sci Science. 2023;35(1):73-83. DOI: https://doi.org/10.5935/2965-2774.20230374-en
11. Curtis JR, Engelberg RA. Nurse activities for communicating with families (Nacf) [Internet]. University of Washington; s.f. http://depts.washington.edu/eolcare/pubs/wp-content/uploads/2011/09/nacf.pdf
12. Downey L, Engelberg R, Shannon Sarah E, Curtis R. Measuring intensive care nurses’ perspectives on family-centered end-of- life care: Evaluation of 3 questionnaires. American Journal of Critical Care. 2006;15(6):568-79. DOI: https://doi.org/10.4037/ajcc2006.15.6.568
13. Cabrera LS, Quintana BY, Alonso JM, Ramírez Montesdeoca F, Marrero IR, Susilla Pérez De La Blanca A. Actividades de comunicación del personal de enfermería con los familiares de pacientes ingresados en una unidad de cuidados intensivos. Enferm Clin [Internet]. 2009;19(6):335-9. DOI: https://doi.org/10.1016/j.enfcli.2009.02.007 [13]
14. Achury Beltrán LF, Ramos Garzón JX. Validación de un instrumento para medir la comunicación con la familia del paciente crítico. Avances en Enfermería. 2024;42(1). DOI: https://doi.org/10.15446/av.enferm.v42n1.110362 [14]
15. Achury Saldaña DM, Achury Beltrán LF, Rodríguez Colmenares SM, Alvarado Romero HR, Cavallo E, Ulloa AC, et al. Professional profile and work conditions of nurses working in intensive care units: A multicentre study. J Clin Nurs [Internet]. 2022;31(11-12):1697-708. DOI: https://doi.org/10.1111/jocn.16026 [15]
16. Murillo Pérez MA, López López C, Torrente Vela S, Morales Sánchez C, Orejana Martín M, García Iglesias M, et al. Percepción de las enfermeras sobre la comunicación con la familia de pacientes ingresados en un servicio de medicina intensiva. Enferm. Intensiva [Internet]. 2014;25(4):137-45. DOI: https://doi.org/10.1016/j.enfi.2014.09.001 [16]
17. Yoo HJ, Lim OB, Shim JL. Critical care nurses’ communication experiences with patients and families in an intensive care unit: A qualitative study. PLoS One. 2020;15(7): e0235694 DOI: https://doi.org/10.1371/journal.pone.0235694 [17]
18. Parada SRG, Castaño ÁMH, Robayo CLM, Restrepo MCT, Herrera JDB, Fernández KDN, et al. Nursing interventions to meet information needs of family members of critically ill patients. Revista Cuidarte. 2021;12(2).
19. Roze des Ordons AL, Stelfox HT, Sinuff T, Grindrod-Millar K, Sinclair S. Exploring spiritual health practitioners’ roles and activities in critical care contexts. J Health Care Chaplain. 2022;28(1):41-62. DOI: https://doi.org/10.1080/08854726.2020.1734371
20. Bautista Rodríguez LM, Arias Velandia MF, Carreño Leiva ZO. Percepción de los familiares de pacientes críticos hospitalizados respecto la comunicación y apoyo emocional. Revista Cuidarte [Internet]. 2016;7(2):1297-309. DOI: https://doi.org/10.15649/cuidarte.v7i2.330
21. Reifarth E, Garcia Borrega J, Kochanek M. How to communicate with family members of the critically ill in the intensive care unit: A scoping review. Vol. 74, Intensive and Critical Care Nursing. Churchill Livingstone; 2023. DOI: https://doi.org/10.1016/j.iccn.2022.103328
22. Casabella García C, Pálizas F, Solano Rueda CA, Guantay ME, Garay CD. Cambios en las visitas a cuidados intensivos durante la pandemia COVID-19. Medicina (Buenos Aires) [Internet]. 2020;80(6):119-20. http://www.scielo.org.ar/scielo.php?script=sci_arttext&pid=S0025-76802020001000119
23. Duffield C, Gardner G, Doubrovsky A, Adams M. Does education level influence the practice profile of advanced practice nursing? Collegian [Internet]. 2021;28(3):255-60. DOI: https://doi.org/10.1016/j.colegn.2020.08.006 [23]
24. Nassiri P, Bakhtom S, Borgheipour H. The Relationship between Shift Work and Burnout among ICU Nursing Staff in Hospitals of Shahid Beheshti University of Medical Sciences. Novelty in Biomedicine [Internet]. 2019;4:181-6. https://eds-s-ebscohostcom.ezproxy.javeriana.edu.co/eds/pdfviewer/pdfviewer?vid=3&sid=7c10e049-6af1-4965-bcfc-1e25fce5e284%40redis
25. Ejebu OZ, Dall’Ora C, Griffiths P. Nurses’ experiences and preferences around shift patterns: A scoping review. PLoS One. 2021;16(8):e0270446. DOI: https://doi.org/10.1371/journal.pone.0270446
26. Edward KL, Galletti A, Huynh M. Enhancing communication with family members in the intensive care unit: A mixed-methods study. Crit Care Nurse. 2020;40(6):23-32. DOI: https://doi.org/10.4037/ccn2020595