
|
|
ARTICLE

José Arturo Medina-Fernández 1
Isaí Arturo Medina-Fernández 2
Antonio Vicente Yam-Sosa 3
Julia Alejandra Candila-Celis 4
1 Universidad Autónoma del Estado de Quintana Roo, México
![]() 0000-0003-0588-9382
0000-0003-0588-9382
![]() josue.medina@uqroo.edu.mx
josue.medina@uqroo.edu.mx
2 https://orcid.org/ Universidad Autónoma de Coahuila, México
![]() 0000-0003-2845-4648
0000-0003-2845-4648
![]() isai-medina@uadec.edu.mx
isai-medina@uadec.edu.mx
3 Universidad Autónoma de Yucatán, México
![]() 0000-0002-7499-1009
0000-0002-7499-1009
![]() antonio.yam@correo.uady.mx
antonio.yam@correo.uady.mx
4 Universidad Autónoma de Yucatán, México![]() 0000-0003-2524-061X
0000-0003-2524-061X
![]() julia.candila@correo.uady.mx
julia.candila@correo.uady.mx
Theme: Care processes and practices
Contribution to the discipline: The Situation-Specific Theory proposal contributes to the nursing disciplinary knowledge, given that it provides comprehension in caring for the elderly with chronic non-malignant pain. This theoretical perspective enriches the nursing practice and offers a solid base to design personalized and holistic interventions, thus optimizing pain management, promoting the comprehensive well-being of elderly individuals.
Received: 21/07/2024
Sent to peers: 27/09/2024
Approved by peers: 17/03/2025
Accepted: 27/03/2025
To reference this article / Para citar este artículo / Para citar este artigo Medina-Fernández JA, Medina-Fernández IA, Yam-Sosa AV, Candila-Celis JA. Trajectory of Living with Chronic Non-malignant Pain in Older Adults: Situation-Specific Theory. Aquichan. 2025;25(3):e2538. DOI: https://doi.org/10.5294/aqui.2025.25.3.8
Abstract
Introduction: The design of a nursing-specific theory will support improving care from a gerontological-geriatric approach. Given the rise of the elderly population and the diverse pathological conditions that chronic pain triggers, this theory integrates physical-functional, cognitive-psychological and socio-family aspects, which support care with this theoretical approach.
Objective: To construct a situation-specific theory that explains the phenomenon of the trajectory of the disease that causes chronic non-malignant pain in the elderly.
Methodology and Materials: This was a five-stage theoretical study: 1) theoretical construction, 2) construction of principal concepts, 3) construction of the theoretical articulation, 4) construction of propositions and empirical indicators to establish causal relationships, and 5) construction of evidence for the nursing practice.
Results: The antecedent is derived from Weiner and Dodd's Nursing Trajectory theory. Four metaparadigm concepts and fourteen main concepts were described, a theoretical articulation was developed, eight propositions were constructed, and seven empirical indicators were developed to establish causal relationships that function as evidence for the practice. The scope of the theory and the implications for the nursing practice are also presented.
Conclusion: This theory allows identifying the process and the necessary considerations to accompany an elderly person living with chronic non-malignant pain. It includes the organization, temporality, identity, and body as fundamental concepts. This theory's proposal establishes a precedent to apply these concepts in gerontological-geriatric consultations and interventions.
Keywords (Source: DeCS): Elderly; chronic pain; nursing theory; geriatric nursing; nursing
Resumen
Introducción: El diseño de una teoría específica de enfermería apoyará el mejoramiento de la atención desde un enfoque geronto-geriátrico. Dado el aumento de la población de adultos mayores y las diversas condiciones patológicas que desencadena el dolor crónico, esta teoría integra aspectos físicos-funcionales, cognitivos-psicoló-gicos y sociofamiliares, que fundamentan los cuidados con este enfoque teórico.
Objetivo: Construir una teoría de situación específica que explique el fenómeno de la trayectoria de la enfermedad que ocasiona dolor crónico no maligno en el adulto mayor.
Metodología: Estudio teórico que se realizó en cinco etapas: 1) construcción teórica, 2) construcción de los conceptos principales, 3) construcción de la articulación teórica, 4) construcción de proposiciones e indicadores empíricos para el establecimiento de relaciones de causalidad y 5) construcción de evidencia para la práctica en enfermería.
Resultados: El antecedente se deriva de la teoría de la trayectoria de la enfermería de Wiener y Dodd. Se describieron cuatro conceptos de metaparadigmas y 14 principales, se hizo el desarrollo de una articulación teórica, de la construcción de ocho proposiciones y de siete indicadores empíricos para establecer relaciones de causalidad que funcionan como evidencia para la práctica; también se presenta el alcance de la teoría y las implicaciones para la práctica de enfermería.
Conclusión: Esta teoría permite identificar el proceso y las consideraciones necesarias para acompañar a una persona adulta mayor que vive con dolor crónico no maligno. Incluye la organización, la temporalidad, la identidad y el cuerpo como conceptos fundamentales. La propuesta de esta teoría establece un precedente para la aplicación de estos conceptos en consultas e intervenciones geronto-geriátricas.
Palabras clave (Fuente: DeCS): Anciano; dolor crónico; teoría de la enfermería; enfermería geriátrica; enfermería
Introdução: A formulação de uma teoria específica de enfermagem contribuirá para a melhoria do cuidado sob uma abordagem gerontogeriátrica. Diante do aumento da população idosa e das diversas condições patológicas desencadeadas pela dor crônica, essa teoria integra aspectos físico-funcionais, cognitivo-psicológicos e socio-familiares, que fundamentam o cuidado com base nessa abordagem teórica.
Objetivo: Construir uma teoria de situação específica que explique o fenômeno da trajetória da doença causadora da dor crônica não maligna em idosos.
Materiais e método: Estudo teórico realizado em cinco etapas: 1) construção teórica; 2) construção dos conceitos principais; 3) construção da articulação teórica; 4) construção de proposições e indicadores empíricos para o estabelecimento de relações de causalidade; e 5) construção de evidências para a prática de enfermagem.
Resultados: O ponto de partida deriva da teoria da trajetória da enfermagem, de Wiener e Dodd. Foram descritos quatro conceitos de metaparadigma e 14 principai. Foi desenvolvida uma articulação teórica, com a construção de oito proposições e sete indicadores empíricos voltados à identificação de relações de causalidade que servem como evidência para a prática. Também são apresentados o escopo da teoria e suas implicações para a prática de enfermagem.
Conclusão: Essa teoria permite identificar o processo e as considerações necessárias para acompanhar um idoso que vive com dor crônica não maligna. Inclui organização, temporalidade, identidade e corpo como conceitos fundamentais. A proposta dessa teoria estabelece um precedente para a aplicação desses conceitos em consultas e intervenções gerontogeriátricas.
Palavras-chave (Fonte DeCS): Idoso; dor crônica; teoria de enfermagem; enfermagem geriátrica; enfermagem
Introduction
Comprehension acquired by the nursing profession regarding chronic non-malignant pain in the elderly has progressed notably in recent decades; however, there are still major gaps that warrant the formulation of a Situation-Specific Theory (SST). Chronic pain in this age group is a complex, multidimensional, and subjective experience, which depends on physiological, psychological, social, and cultural characteristics 1. Despite emphasizing the seriousness of this phenomenon, there is an underlying reflection on the meaning of living with chronic non-malignant pain and how this is translated internally and externally.
Within the scope of existing theories, Roy's Adaptation Model and Larson's Theory of Symptom Management have been proposed to explain responses to chronic pain in the elderly, focusing on coping and adaptation 2. However, these theories are limited in scope for capturing specific aspects of the prolonged and dynamic experience of pain in older adults because they do not inquire in depth into changes over time and into the social implications. The lack of an SST that encompasses the experience of living with chronic non-malignant pain in elderly individuals restricts knowledge and development of individualized nursing interventions. Hence, formulating an SST permits understanding this condition and enables developing care models for the elderly, the frail, and those with even more complex needs.
Thus, the disease produced by chronic non-malignant pain is of great interest in care processes for the geriatric nursing practice. For this, the functional modifications caused by pain are identified, as well as the changes that occur in the elderly from a physical, psychological, family, and social perspective. Evaluating these aspects in the elderly permits understanding the impact of chronic non-malignant pain on their lives.
Currently, from the social point of view, a culture has been developed in pain management from a symptomatic approach; therefore, its treatment is pharmacological. The SST is a theoretical proposal that helps nursing professionals understand and act effectively on pain management.
For people living with chronic non-malignant pain, this condition imposes a series of challenges that affect multiple aspects of life, from a deterioration in quality due to functional limitation and social isolation, to the appearance of psychiatric comorbidities, like depression and anxiety. Likewise, these people often face economic and employment obstacles that contribute to a greater socioeconomic burden associated with this condition 1,3.
From an international point of view, chronic pain is a significant concern for public health, given that it affects between 25 and 29 % of the global population. In Latin America, the condition's incidence is high, affecting from 27 to 42 % of the population, almost double the global incidence. In Mexico, it is estimated to affect between 25 and 27 °% of the population, equivalent to nearly 40 million people; it is striking that only 14 °% of those suffering from chronic pain receive treatment 4-7.
Some diseases, such as arthritis, lumbar pain, fibromyalgia, cancer, neuropathies, and fractures, can cause chronic non-malignant pain as they evolve 8,9. Likewise, this type of pain is frequent in the elderly population, as indicated by the National Study on Health and Aging in Mexico, which shows that 41.5 % of adults over 50 years of age reported suffering pain, with this being more frequent in women than in men (48.3 % vs. 33.6 %), a higher figure in the elderly group 10,11.
Consequently, the concepts that integrate the SST are based on the disease trajectory and, from a sociological perspective, on the relations that affect the exercise of living with them, whose influence is derived from the work by Corbin and Strauss, who observed in a qualitative study in individuals with cancer that this disease had discernible phases or stages that could be identified through significant changes in problems, challenges, or activities -so the person's physical state and the socio-psychological consequences of the disease and treatment were the central themes at all measurement points throughout the research.
That said, this SST also supports nursing prescription by providing a framework that guides the assessment, intervention, and follow-up of the older adult, recognizing the disease as a complex and individualized experience. From this, the nursing prescription is based on strategies that address comprehensive pain management, promoting self-management, emotional well-being, and adaptation to the individual's chronic condition in their journey of living with pain.
Hence, within this context, the role played by the nursing staff is highly valued. Nurses are a fundamental link between patients and professional health personnel; moreover, their responsibility is to relieve physical pain through effective techniques and analgesics, in addition to assessing and providing gerontological-geriatric consultation, seeking to implement pharmacological and non-pharmacological interventions to make a significant difference in the perception of pain and the overall well-being of people living with this condition. The general objective proposed in this work was to construct an SST that explains the phenomenon of the disease that causes chronic non-malignant pain in the elderly, derived from Wiener and Dodd's illness trajectory intermediate theory.
Methodology
Construction of the SST used the five steps of the design of theorizations by Oliveira et al.12; it must be specified that this design is a model used by nursing professionals to develop specific theories that address the particular needs and situations of patients, based on practical evidence. This model includes the observation and analysis of specific clinical situations in the following stages: (i) the theoretical construction approach, (ii) definition of principal concepts, (iii) construction of the theoretical articulation, (iv) construction of propositions and empirical indicators to establish causal relationships, and (v) evidence for the nursing practice 12.
Definition of the approach
The definition of the main concepts of this intermediate-range theory was made based on the analysis of the disease trajectory, whose pathologies cause non-malignant pain. For this purpose, the scientific production carried out by renowned authors on the subject was reviewed, both in quantitative and qualitative designs. These antecedents permitted defining the approach based on the experiences of the elderly living with chronic pain, besides considering physical, functional, cognitive, psychological, family, and social aspects 12.
Construction of principal concepts
This phase incorporated conceptual elements, that is, definitions that permitted describing them specifically, developed based on Wiener and Dodds' Illness Trajectory Intermediate Theory, adapting them to the specific situation, allowing to identify the reference concepts to design the theoretical article and its propositions, aiming to convert them into a prescriptive theory focused on gerontological-geriatric care for the elderly living with chronic non-malignant pain. This theory, which can be applied in pharmacological and non-pharmacological interventions based on the analysis of the gerontological-geriatric consultation-assessment, focuses on functional, cognitive, and social aspects 12.
Construction of the theoretical articulation.
To facilitate understanding the SST, a pictorial diagram or theoretical articulation was designed from the concepts proposed, seeking to relate and explain those that comprise the theory 12.
Construction of propositions
Through a reasoning exercise about the relationship and articulation of the concepts that integrate the theory, propositions were formulated based on scientific evidence and practice 12.
Figure 1 Theoretical articulation of the SST of disease trajectory in the elderly living with chronic non-malignant pain
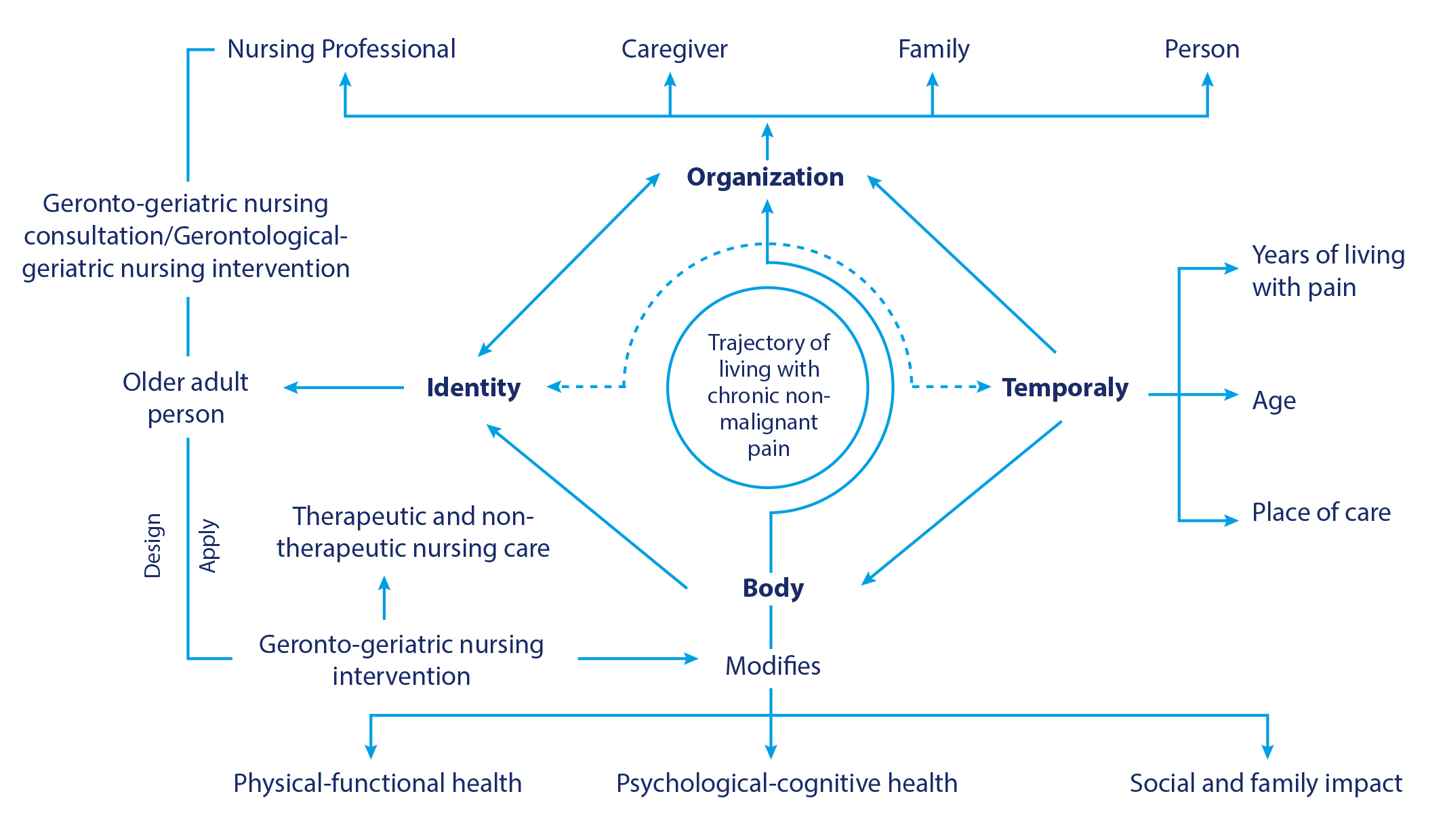
Source: Based on the illness trajectory theory developed by Carolyn L. Wiener and Marilyn J. Dodd.
Empirical indicators to establish causal relationships and evidence for the nursing practice
In this last stage, we established and described causal relationships among the concepts that configure the disease trajectory that causes chronic non-malignant pain. This stage permitted examining with an operational vision the phenomenon of interest and, therefore, describing in detail the gerontological-geriatric nursing actions. Specifically, this stage served to establish causal relationships among the concepts of the theory and to present useful evidence for the nursing practice.
To achieve the foregoing, it was necessary to introduce instruments and scales that, in the results of their application, showed the causal relationships among the concepts from a quantitative perspective. This stage was important because it provided the opportunity to understand the phenomenon from a qualitative approach. It also allowed explaining the scope of SST and its possible implications for the nursing science research and practice.
Results
The analysis of studies found on the evidence search was conducted in several countries. These studies addressed some variables from a qualitative perspective, with pathologies that cause chronic non-malignant pain, such as arthritis, fibromyalgia, diabetes, low-back pain, and arthrosis; these include: the experience of living with pain, the effects of life after diagnosis, adaptation to change, the limitations of living with benign chronic pain, strategies to reduce it, behavioral changes, identification of negative feelings, isolation, physical exhaustion, crises in daily life, socio-family modifications, and the negative/positive participation of health staff 13-17.
It was also observed that the elderly have moderate beliefs, related with age, about the origin of pain, compared with those who believe that pain has a pathological cause and are more likely to seek help because they are convinced that they have better control and courage in the face of pain, and are not willing to reveal it to others 18-22.
Likewise, it was found that the elderly individual's independence influences the search for professional health treatment and the behavior to be able to endure and "learn to live with pain." Over time, participants learn to adapt, one day at a time, to balance activities, thoughts, and emotions, trying not to be a burden to the family and others, enjoying and appreciating pleasurable moments that help them cope with their ailments 23-25.
Consequently, the SST proposed is based on Wiener and Dodd's illness trajectory intermediate theory, which includes the physical components of the disease and the organization of all the work conducted throughout such, that is, its trajectory is theoretically different from the course, because this is not only limited to the person suffering from pain, but includes the family and the health professionals who participate in their care 26-28.
The organization's participants have different types of work; therefore, the person living with the disease is central to the disease trajectory. The burden implied by living with pain gives rise to consequences and impacts on the lives of those involved, as it affects the course of the disease and the fate of the sick.
Also, the elderly are recognized as central actors in managing their condition, given that they are the ones who execute the actions to cope with the impact of the disease in multiple contexts, including the biographical (related to their self-perception) and the sociological (linked to their social relationships). From this perspective, control of alterations (or coping with uncertainty) implies interactions with several participants in the organization (the sick person, family, and health professionals), as well as some external social conditions. Given the complexity of said interactions in multiple contexts and with numerous participants, the older person experiences modifications in coping because non-malignant pain is quite variable and dynamic in each individual 29-31.
The SST has a descriptive, explanatory, and prescriptive scope. At the descriptive level, the disease process that leads to chronic pain is characterized, addressing the alteration of functionality and the physical, psychological, and socio-family changes in older adults. From an explanatory approach, the SST identifies chronic non-malignant pain as the core of these transformations and analyzes the factors that influence the disease trajectory.
In the prescriptive level, the theory not only recognizes the need for intervention but also establishes concrete strategies to modify the disease trajectory. From the experience and the severity of pain, it proposes specific gerontological-geriatric care approaches that permit improving the functionality of the elderly person and preventing the appearance of geriatric syndromes associated with chronic non-malignant pain. This is achieved by implementing differentiated interventions, like functional rehabilitation programs, psychosocial support through mutual support groups, as well as pharmacological and non-pharmacological adjustments.
Concepts of metaparadigms
Human being
It is the older adult living with chronic non-malignant pain due to an illness whose impact is physical, psychological, and social; this is characterized by changes in daily life, decreased functionality, modifications in behavior and feelings, with socio-family impact and a negative perception of their treatment towards pain reduction.
Health
Human response of the elderly to change in daily life due to increased chronic non-malignant pain, with direct impact on their functionality, psychological, and socio-family modifications.
Nursing
The science that identifies changes in chronic non-malignant pain due to disease deterioration in the elderly; its focus is on comprehensive geriatric assessment, that is, providing nursing care with both therapeutic and non-therapeutic approaches, avoiding the loss of functionality, physical, psychological, and social changes, and allowing adaptation to their condition and greater integration with the family and society.
Environment
The environment is comprised of the individual, health professionals, society, the family, and the caregiver, among whom there is a direct relationship with the behavior of chronic pain care, which influences the adaptation to life by the affected person, their functionality, physical changes, psychological condition, and socio-family relations.
World vision
This SST presents a vision of reciprocal interaction in which the elderly with chronic non-malignant pain are considered holistic, active, and interactive human beings with their environment. From this perspective, the older adult is not a passive subject of care, but responds and adapts to interactions with the caregiver, family, and nursing professionals. Said dynamic allows them to face their reality in a multidimensional manner, considering physiological, emotional, and sociocultural factors that modulate their experience of pain. Also, their response and adaptation are determined by the context in which they live and the surrounding conditions, which requires a comprehensive nursing approach, based on continuous assessment and planning of specific interventions 6.
Definition of principal concepts
Trajectory of living with chronic non-malignant pain: individual experiences of the older adult, from the diagnosis of the disease, whose main symptom is chronic non-malignant pain, derived from a disease that is not life-threatening, but which produces physical, psychological, and social changes, and modifies the person's daily life.
Chronic non-malignant pain: pain discomfort in the elderly, of pathological origin, which is not life-threatening, but which is characterized by a duration of more than three months and does not improve despite the treatments performed.
Organization as an older adult person: an individual who is ≥ 60 years of age, who interacts and lives in society while maintaining an sense of self; who has a conscious and rational legal and moral notion, with the capacity for discernment and to respond for their own actions.
Organization as family: a group of people who live under the same roof, or not, as an older adult, who suffers from chronic non-malignant pain, with whom they share feelings that unite and agglutinate them; they are organized into fixed roles, have blood ties or not, and maintain a specific economic and social existence.
Organization as caregiver: a person who provides assistance to another person living with chronic non-malignant pain and in need of help with self-care. This person may be a family member, friend, or member of a faith-based organization that provides assistance in the home, hospital, or other healthcare setting.
Organization as a nursing professional: a person who autonomously and collaboratively assumes nursing care for the elderly living with chronic non-malignant pain in all settings.
Identity: perception of the older adult living with chronic non-malignant pain at a given moment, which unifies multiple personal attributes and is situated in the mind and body.
Gerontological-geriatric nursing consultation: nursing action characterized by identifying the risk factors for functional dependence of the elderly living with chronic non-malignant pain by applying a physical, functional, psychological and social assessment to avoid them.
Gerontological-geriatric nursing intervention: therapeutic care planned and performed based on the gerontological-geriatric consultation to improve or maintain the physical-functional, psychological-cognitive, and socio-family health of the elderly living with chronic non-malignant pain.
Temporality: situation or condition produced during a limited time interval whose end is uncertain. It may be modified by factors such as age, years living with chronic non-malignant pain, and the place where the sick person lives.
Body: it is the object transformed during the process of caring for the elderly living with chronic non-malignant pain. This can be modified by physical, functional, psychological, cognitive aspects and by socio-family relations, expressing signs of wanting to be cared for and listened to. Within this context, the subjects are the ones who request care, so that it allows them to express their needs and generate an interrelationship that favors their recovery, where both bodies (care-caregiver) develop their own communication codes, and nursing professionals will use their senses to carry out this process of interaction and care.
Physical-functional health: the degree to which the elderly living with chronic non-malignant pain maintain their physical well-being, walking speed, limb strength and balance, in addition to the quality with which they assume social roles and whether their intellectual and emotional state, social activity and attitude towards life are modified according to the degree of chronic pain.
Psychological-cognitive health: psychological-cognitive evaluation of the presence of depressive symptoms, anxiety, self-isolation, risk of cognitive decline, loss of attention functions, speed of information processing, and memory of the elderly with these pathologies.
Social and family impact: changes in daily life, family and social dynamics, as a result of chronic non-malignant pain in the elderly.
Proposal of theoretical articulation
Construction of propositions
Eight propositions were developed with different theoretical applications ranging from the descriptive to the prescriptive.
With regards to the organization, in the elderly living with chronic non-malignant pain, the family, caregivers, and nursing professionals are considered care actors.
With respect to the disease trajectory, the elderly, according to age, time living with chronic pain, and place of care, have modifications in functionality, walking speed, limb strength, and balance.
Regarding the years living with the disease causing the chronic non-malignant pain, changes in everyday life at home and modifications in the person's family dynamics are observed, in addition to suffering from family and social self-isolation.
Nursing professionals apply the gerontological-geriatric assessment in the elderly who live with chronic non-malignant pain, considering their identity as part of the care.
The comprehensive geriatric assessment serves as a priority activity for nursing staff, as it allows identifying changes in physical-functional, psychological-cognitive, and socio-family relationships, whose purpose is to design and implement care according to the effects of the older adult's experience with chronic non-malignant pain.
Therapeutic nursing care allows the elderly to diminish the level of chronic non-malignant pain, permitting improvement in their functional, psychological, and social activity.
Non-therapeutic nursing care, such as manual, natural, oriental, relaxation, and complementary therapies, contributes to diminishing chronic non-malignant pain in the elderly, allowing for improvements in their functional, psychological, and social activity.
Nursing generates support groups in which the elderly with chronic pain share experiences of therapeutic and non-therapeutic outcomes to create social networks that help them integrate into their daily and social lives.
Empirical indicators to establish causal relationships and evidence for practice.
The analysis of empirical indicators addressed the SST components individually, given that these conjugate the physical-functional, psychological-cognitive, and socio-family, in addition to everything observed from the individual experience, without considering age, age group of the older individual, the caregiver, relative, or nursing professional.
The following describes some indicators that can help test this SST, which offers an opportunity to consider the factors that tend to be affected by chronic non-malignant pain in the elderly.
The Short Form McGill Pain Questionnaire (SF-MPQ) is a self-report measure of the quality of benign or malignant pain, validated in English and Spanish, which is composed of 15 descriptors; representing both the sensory and affective senses, it describes the severity of the experience of living with pain 32.
The Pain Disability Questionnaire (PDI) is a self-report measure validated in English, consisting of seven items that assess disability from benign and malignant chronic pain in seven areas: family, occupation, sexual relations, social activities, recreation, self-care, and life support. Participants are asked to indicate their disability in each of the seven areas 33.
The Pain Catastrophizing Scale (PCS) is a self-report measure validated in Spanish and has 13 items related to the catastrophizing of benign and malignant chronic pain. Individuals are instructed to reflect upon their pain experience and to indicate the degree to which they experience thoughts or feelings during the pain, which allows calculating three subscale scores: rumination, magnification, and helplessness 34.
The Chronic Pain Coping Inventory (CPCI) is a 65-item scale of cognitive and behavioral coping, often used as part of multidisciplinary pain treatment. Each element represents a coping strategy; thereby, individuals are asked to indicate the number of days they used the strategy to confront pain during the previous week. This has eight subscales that represent the use of different types of coping strategies, like protection, rest, requesting help, relaxation, persistence in the task, exercise or stretching, seeking social support, and coping self-affirmations 35.
The Multitasking Preference Inventory (MPI) scale is a measurement of 60 items designed in English, which permits evaluating multiple psychosocial functioning aspects in patients with benign and malignant chronic pain. This comprises three parts, the first evaluates the impact of pain and is composed of five subscales: interference, support, pain intensity, self-control, and negative mood. The second evaluates the responses of significant persons and produces three subscales: punishment responses, solicitous responses, and distraction responses. The last part evaluates the activities and has four subscales related to the level of the patient's activity: household tasks, outdoor work, activities outside the home, and social activities 36.
The Psychological Inflexibility in Pain Scale (PIPS-J) was developed to measure psychological rigidity in relation to chronic pain. This scale is validated in Japanese and is applied to any type of pain. It assesses avoidance behaviors related to pain and levels of cognitive fusion related to it; however, it has only been applied in that country's population 37.
Lastly, among other indicators that can complement information through qualitative research with a phenomenological approach, as it brings together the experiences of older adults, there is a study conducted in Mexico in which an exact description was found of what the wear and tear of living with pain represents, the changes in daily life, the alternatives used to relieve pain, and the effects on the social environment 13.
Scope of the situation-specific theory
The scope of this theory is of great importance in nursing, given that this SST with a comprehensive approach considers and analyzes all the aspects that affect the elderly living with chronic non-malignant pain, it also considers the factors of the caregiver, the family, and the nursing staff as part of their care organization.
Thus, therapeutics is applied in nursing with a concept called gerontological-geriatric intervention, which is addressed according to the outcomes of the gerontological-geriatric consultation of the older adult in which a physical, functional, cognitive, and social assessment is performed; according with this assessment a specific intervention is planned for the adult, whether functional or not, according to the level of risk identified, to point out the risk factors for functional dependence and avoid, reduce or delay the level of dependence in older adults. It also promotes the incorporation of nursing consultancy as a strategy to contribute to modifying the physical-functional, psychological-cognitive, and socio-family components in the elderly who live with chronic pain in the different levels of care of the National Health System.
Implications
The proposed SST can be corroborated from a quantitative perspective through the use or generation of new validated scales that help identify how the proposed theoretical articulation interacts and complements it with a qualitative perspective to deepen the feelings of the nursing professionals, caregivers, family, and the older adult living with chronic pain.
Likewise, it is deemed necessary to address the gerontological-geriatric consultations and interventions from the nursing perspective, given that these allow identifying the risks and factors that alter the life of the person living with pain, to generate individualized interventions according to the older individual's level of functionality, and being able to integrate them more into life.
Conclusions
The scope of this SST transcends the individual level, integrates a holistic approach that considers the impact of pain in the family dynamics, the role of the primary caregiver, participation by the nursing professional, and the influence of contextual variables, such as the care setting (home, institutional or community).
From this perspective, the SST provides a theoretical framework for the gerontological-geriatric consultation and intervention, facilitating the formulation of strategies based on the comprehensive evaluation of the elderly. This includes pain management, preservation of functionality, prevention of geriatric syndromes, and implementation of personalized care plans that consider age, disease evolution, socio-family conditions, and resources available in the care context. Thus, this theory not only contributes to the development of geriatric nursing knowledge but also guides the clinical practice toward more effective and contextualized interventions.
Referencias
1. Kraft K, Backmund T, Eberhart L, Schubert AK, Dinges HC, Hagen MK, et al. Does opioid therapy enhance quality of life in patients suffering from chronic non-malignant pain? A systematic review and meta-analysis. Br J Pain. 2024;18(3):227-42. DOI: https://doi.org/10.1177/20494637231216352
2. Alligood M. Modelos y teorias en enfermeria. 9a ed. Espana, Elsevier; 2028. p. 1-580
3. Caceres-Matos R, Gil-Garcia E, Barrientos-Trigo S, Porcel-Galvez A, Cabrera-Leon A. Consequences of Chronic Non-Cancer Pain in adulthood. Scoping Review. Rev Saude Publica. 2020;54:39. DOI: https://doi.org/10.11606/s1518-8787.2020054001675
4. Wang L, Ye H, Li Z, Lu C, Ye J, Liao M, et al. Epidemiological trends of low back pain at the global, regional, and national levels. European Spine Journal. 2022;31(4):953-62. DOI: https://doi.org/10.1007/s00586-022-07133-x
5. Sa KN, Moreira L, Baptista AF, Yeng LT, Teixeira MJ, Galhardoni R, et al. Prevalence of chronic pain in developing countries: systematic review and meta-analysis. Pain Rep. 2019;4(6):e779. DOI: https://doi.org/10.1097/PR9.0000000000000779
6. Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273-83. DOI: https://doi.org/10.1016/j.bja.2019.03.023
7. Covarrubias A, Guevara U, Betancourt J, Gutierrez C, Cordova J. Epidemiologia del dolor cronico en Mexico. Revista Mexicana de Anestesiologia. 2010;33(4):1-7. https://www.medigraphic.com/pdfs/rma/cma-2010/cma104e.pdf
8. Morales-Fernandez A, Jimenez Martin JM, Vergara-Romero M, Morales-Asencio JM, Mora-Bandera AM, Gomez-Ortigosa MI, et al. Gender differences in perceived pain and health-related quality of life in people with chronic non-malignant pain: a cross-sectional study. Contemp Nurse. 2021;57(3-4):280-9. DOI: https://doi.org/10.1080/10376178.2021.1999836
9. Kovačević I, Majerić Kogler V, Krikšić V, Ilić B, Friganović A, Ozimec Vulinec Š, et al. Non-Medical Factors Associated with the Outcome of Treatment of Chronic Non-Malignant Pain: A Cross-Sectional Study. Int J Environ Res Public Health. 2022;19(5):2881. DOI: https://doi.org/10.3390/ijerph19052881
10. Covarrubias A. Las clinicas del dolor en Mexico. Revista Mexicana de Anestesiologia. 2008;31(1):1-5. https://www.medigraphic.com/pdfs/rma/cma-2008/cma081k.pdf
11. Barragan A, Mejia S, Gutierrez M. Dolor en adultos mayores de 50 años: prevalencia y factores asociados. Salud Publica de Mexico. 2007;49(4):1-7. DOI: https://doi.org/10.1590/S0036-36342007001000008
12. de Oliveira Lopes MV, da Silva VM, Herdman TH. Causation and Validation of Nursing Diagnoses: A Middle Range Theory. Int J Nurs Knowl. 2017;28(1):53-9. DOI: https://doi.org/10.1111/2047-3095.12104
13. Ruiz-Aguilar K, Chan-Castro V, Hernandez-Gomez G, Cab- Lopez A, Espadas-Uuh J, Medina-Fernandez J. Vivir con dolor cronico desde la experiencia de adultos mayores con enfermedades cronico-degenerativas. Horiz Enferm. 2021;32(3):297-305. DOI: https://doi.org/10.7764/Horiz_Enferm.32.3.297-305
14. Vader K, Doulas T, Patel R, Miller J. Experiences, barriers, and facilitators to participating in physical activity and exercise in adults living with chronic pain: a qualitative study. Disabil Rehabil. 2021;43(13):1829-37. DOI: https://doi.org/10.1080/09638288.2019.1676834
15. Tinnirello A, Mazzoleni S, Santi C. Chronic Pain in the Elderly: Mechanisms and Distinctive Features. Biomolecules. 2021;11(8):1256-1236. DOI: https://doi.org/10.3390/biom11081256
16. Miaskowski C, Blyth F, Nicosia F, Haan M, Keefe F, Smith A, et al. A Biopsychosocial Model of Chronic Pain for Older Adults. Pain Medicine. 2020;21(9):1793-805. DOI: https://doi.org/10.1093/pm/pnz329
17. Dagnino A, Campos M. Chronic Pain in the Elderly: Mechanisms and Perspectives. Front Hum Neurosci. 2022;16(1):1-12. DOI: https://doi.org/10.3389/fnhum.2022.736688
18. Iqbal A, Toh L, Knaggs R, Anderson C. Factors promoting self-medication and irrational use of opioids in chronic non-malignant pain management in Pakistan: A qualitative in-depth investigation. International Journal of Pharmacy Practice. 2021;29(Supplement 1):i32-3. DOI: https://doi.org/10.1093/ijpp/riab015.039
19. Hamilton M, Gnjidic D, Christine-Lin CW, Jansen J, Weir K, Shaheed C, et al. Opioid deprescribing: Qualitative perspectives from those with chronic non-cancer pain. Research in Social and Administrative Pharmacy. 2022;18(12):4083-91. DOI: https://doi.org/10.1016/j.sapharm.2022.07.043
20. Kovačević I, Majerić-Kogler V, Krikšić V, Ilić B, Friganović A, Ozimec-Vulinec Š, et al. Non-Medical Factors Associated with the Outcome of Treatment of Chronic Non-Malignant Pain: A Cross-Sectional Study. Int J Environ Res Public Health . 2022;19(5):2881. DOI: https://doi.org/10.3390/ijerph19052881
21. Rufener L, Akre C, Rodondi P, Dubois J. Management of chronic non-cancer pain by primary care physicians: A qualitative study. PLoS One. 2024;19(7):e0307701. DOI: https://doi.org/10.1136/bmjopen-2019-032988
22. Nichols V, Toye F, Eldabe S, Sandhu H, Underwood M, Seers K. Experiences of people taking opioid medication for chronic non-malignant pain: a qualitative evidence synthesis using meta-ethnography. BMJ Open. 2020;10(2):e032988. DOI: https://doi.org/10.1136/bmjopen-2019-032988
23. Schneider J, Algharably E, Budnick A, Wenzel A, Drager D, Kreutz R. Deficits in pain medication in older adults with chronic pain receiving home care: A cross-sectional study in Germany. PLoS One. 2020;15(2):e0229229. DOI: https://doi.org/10.1371/journal.pone.0229229
24. Welsh T, Yang A, Makris U. Musculoskeletal Pain in Older Adults. Medical Clinics of North America. 2020;104(5):855-72. DOI: https://doi.org/10.1016/j.mcna.2020.05.002
25. Teater B, Chonody J. How Do Older Adults Define Successful Aging? A Scoping Review. The International Journal of Aging and Human Development. 2020;91(4):599-625. DOI: https://doi.org/10.1177/0091415019871207
26. Parreira P, Santos-Costa P, Neri M, Marques A, Queiros P, Salgueiro-Oliveira A. Work Methods for Nursing Care Delivery. Int J Environ Res Public Health . 2021;18(4):2088. DOI: https://doi.org/10.3390/ijerph18042088
27. da Silva R, Brandao M, Ferreira M. Integrative Review as a Method to Generate or to Test Nursing Theory. Nurs Sci Q. 2020;33(3):258-63. DOI: https://doi.org/10.1177/0894318420920602
28. Im EO, Meleis AI. Situation-Specific Theories: Philosophical Roots, Properties, and Approach. En: Situation Specific Theories: Development, Utilization, and Evaluation in Nursing. 1a ed. Cham: Springer International Publishing; 2021. p. 13-27. DOI: https://doi.org/10.1007/978-3-030-63223-6_2
29. Wardell DW, Decker SA, Engebretson JC. Healing Touch for Older Adults With Persistent Pain. Holist Nurs Pract. 2012;26(4):194-202. DOI: https://doi.org/10.1097/HNP.0b013e318258528d
30. Ingrid Bergh DSB. Learning to Endure Long-Term Musculoskeletal Pain in Daily Life at Home: A Qualitative Interview Study of the Older Adult’s Experience. J Gerontol Geriatr Res. 2013;02(04). DOI: https://doi.org/10.4172/2167-7182.1000136
31. Gammons V, Caswell G. Older people and barriers to self-reporting of chronic pain. British Journal of Nursing. 2014;23(5):274-8. DOI: https://doi.org/10.12968/bjon.2014.23.5.274
32. Burckhardt C, Bjelle A. A Swedish Version of the Short-Form McGill Pain Questionnaire. Scand J Rheumatol. 1994;23(2):77-81. DOI: https://doi.org/10.3109/03009749409103032
33. Tait RC, Chibnall JT, Krause S. The Pain Disability Index: psychometric properties. Pain. 1990;40(2):171-82. DOI: https://doi.org/10.1016/0304-3959(90)90068-O
34. Osman A, Barrios FX, Kopper BA, Hauptmann W, Jones J, O’Neill E. Factor structure, reliability, and validity of the Pain Catastrophizing Scale. J Behav Med. 1997;20(6):589-605. DOI: https://doi.org/10.1023/A:1025570508954
35. Jensen MP, Turner JA, Romano JM, Strom SE. The chronic pain coping inventory: development and preliminary validation. Pain. 1995;60(2):203-16. DOI: https://doi.org/10.1016/0304-3959(94)00118-X
36. Wittink H, Turk DC, Carr DB, Sukiennik A, Rogers W. Comparison of the Redundancy, Reliability, and Responsiveness to Change Among SF-36, Oswestry Disability Index, and Multidimensional Pain Inventory. Clin J Pain. 2004;20(3):133-42. DOI: https://doi.org/10.1097/00002508-200405000-00002
37. Nagasawa Y, Shibata A, Fukamachi H, Ishii K, Wicksell RK, Oka K. The Psychological Inflexibility in Pain Scale (PIPS): Validity and Reliability of the Japanese Version for Chronic Low Back Pain and Knee Pain. J Pain Res. 2021;14:325-32. DOI: https://doi.org/10.2147/JPR.S287549