|
|
ARTICLE

Victoria Rosado-Berdugo 1
Sandra Henríquez-Figueroa 2
1 Universidad Adventista de Chile, Chile
![]() 0009-0005-8062-5936
0009-0005-8062-5936
![]() victoriarosado@alu.unach.cl
victoriarosado@alu.unach.cl
2 https://orcid.org/ Universidad Adventista de Chile, Chile
![]() 0000-0001-9156-8037
0000-0001-9156-8037
![]() sandrahenriquez@unach.cl
sandrahenriquez@unach.cl
* This paper is derived from the master's dissertation "Efectividad de una intervención anti-estigma hacia pacientes con trastornos mentales en atención primaria Chile" presented to the Universidad Adventista.
** Artículo derivado de la tesis de maestría titulada: Efectividad de una intervención an-ti-estigma hacia pacientes con trastornos mentales en atención primaria Chile, Universidad Adventista. No anexada a repositorio.
***Artigo derivado da dissertação de mestrado intitulada “Efetividade de uma intervenção antiestigma para pacientes com transtornos mentais na atenção primária Chile”, defendida na Universidad Adventista. Não anexada ao repositório.
Theme: Health promotion, well-being and quality of life
Contributions to the field: The findings of this study contribute to refining strategies that allow for the design of more effective interventions to reduce the stigmatization of people with mental disorders. This includes improving healthcare practices, reducing stigmatizing attitudes at the institutional and personal levels, and promoting inclusive and respectful environments. These contributions are essential to ensuring comprehensive and humane care, strengthening the quality of primary health care services.
Received: 14/01/2025
Sent to peers: 11/03/2025
Aprobbed by peers: 03/06/2025
Accepted: 05/06/2025
To reference this article / Para citar este artículo / Para citar este artigo Rosado-Berdugo V, Henríquez-Figueroa S. Effectiveness of an Anti-Stigma Intervention for Patients with Mental Disorders in Primary Care in Chile. Aquichan 2025;25(3):e2537. DOI: https://doi.org/10.5294/aqui.2025.25.3.7
Abstract
Introduction: Stigma towards people with mental disorders hinders access to and the quality of healthcare globally. Reducing this situation among healthcare professionals requires specific interventions.
Objective: To evaluate the effectiveness of an anti-stigma intervention program for patients with mental disorders at a CESFAM in Biobío.
Materials and Methods: A quantitative, analytical, pre-experimental, and longitudinal study was conducted with 40 healthcare professionals selected using stratified random sampling. Participants with more than one year of experience, direct contact with users, and who had attended at least one workshop were included. Those with justified absenteeism from work were excluded. The WHO-HC questionnaire was administered in January 2024 (pre-intervention) and June 2024 (post-intervention). The educational intervention was conducted between March and June 2024. Student's T-test, Wilcoxon's W test, ANOVA, Games-Howell post-hoc tests, and Spearman's Rho coefficient were used for the analysis.
Results: The sample consisted predominantly of women (72.5 %) and professionals aged 30-39 (45 %). The mean questionnaire score was 46.2 (SD ± 8.30) at pre-intervention, remaining unchanged at post-intervention (SD ± 9.4). No statistically significant differences were found in the post-intervention questionnaire.
Conclusion: No reduction in stigma was evident after the intervention. Differences in stigmatizing attitudes were observed based on age and social class, indicating an increase in stigmatizing attitudes associated with years of service; this suggests the use of more targeted approaches to address the problem.
Keywords (Source: DeCS): Stigma; mental health; mental disorders; health professionals; primary health care
Resumen
Introducción: El estigma hacia personas con trastornos mentales dificulta el acceso y la calidad de la atención en salud a nivel global. Para reducir esta situación entre los profesionales de la salud se requieren intervenciones específicas.
Objetivo: Evaluar la efectividad de un programa de intervención anti estigma hacia pacientes con trastornos mentales en un CESFAM de Biobío.
Materiales y Métodos: Estudio cuantitativo, analítico, preexperimental y longitudinal con 40 profesionales de la salud seleccionados mediante muestreo aleatorio estratificado. Se incluyeron participantes con más de un año de antigüedad, contacto directo con usuarios y asistencia a, al menos, un taller. Se excluyó a quienes presentaban ausentismo laboral justificado. Se aplicó el cuestionario OMS-HC en enero de 2024 (preintervención) y en junio de 2024 (posintervención). La intervención educativa se llevó a cabo entre marzo y junio de 2024. Se utilizaron pruebas t de Student, W de Wilcoxon, ANOVA, pruebas post-hoc de Games-Howell y coeficiente de Rho de Spearman para el análisis.
Resultados: La muestra estuvo compuesta mayormente por mujeres (72,5 %) y profesionales de 30-39 años (45 %). El puntaje medio del cuestionario fue de 46,2 (DE ± 8,30) en la preintervención, manteniéndose sin cambios en la postintervención (DE ± 9,4). No se encontraron diferencias estadísticamente significativas en el cuestionario postintervención.
Conclusión: No se evidenció reducción del estigma tras la intervención. Se observaron diferencias en las actitudes estigmatizadoras, según edad, estamento, lo que señala un aumento de actitud estigmatizadora asociada a los años de servicio; esto sugiere el uso de enfoques más específicos para abordar el problema.
Palabras clave (Fuente DeCS): Estigma; salud mental; trastornos mentales; profesionales de la salud; atención primaria de salud
Introdução: O estigma em relação às pessoas com transtornos mentais dificulta o acesso e a qualidade da atenção à saúde em todo o mundo. Para reduzir essa situação entre os profissionais de saúde, são necessárias intervenções específicas.
Objetivo: Avaliar a efetividade de um programa de intervenção antiestigma para pacientes com transtornos mentais em um CESFAM [Centros de Saúde Familiar] no Biobío.
Materiais e métodos: Estudo quantitativo, analítico, pré-experimental e longitudinal com 40 profissionais de saúde selecionados por amostragem aleatória estratificada. Foram incluídos participantes com mais de um ano de experiência, contato direto com os usuários e participação em pelo menos uma oficina. Foram excluídos aqueles que apresentaram ausência justificada no trabalho. O questionário OMS-HC foi aplicado em janeiro de 2024 (pré--intervenção) e em junho de 2024 (pós-intervenção). A intervenção educativa foi realizada entre março e junho de 2024. Para a análise, foram utilizados o teste t de Student, o W de Wilcoxon, a ANOVA, os testes post-hoc de Games-Howell e o coeficiente Rho de Spearman.
Resultados: A amostra foi composta majoritariamente por mulheres (72,5 %) e profissionais com idade entre 30 e 39 anos (45 %). A pontuação média do questionário foi de 46,2 (DP ± 8,30) no pré-intervenção, mantendo-se inalterada no pós-intervenção (DP ± 9,4). Não foram encontradas diferenças estatisticamente significativas no questionário pós-intervenção.
Conclusão: Não houve evidência de redução do estigma após a intervenção. Foram observadas diferenças nas atitudes estigmatizantes, de acordo com a idade e o estamento, o que indica aumento das atitudes estigmatizantes associadas aos anos de serviço. Isso sugere o uso de abordagens mais específicas para resolver o problema.
Palavras-chave (Fonte: DeCS): Estigma; saúde mental; transtornos mentais; profissionais de saúde; atenção primária à saúde
Introduction
According to the 2023 World Mental Health Report, of the Pan American Health Organization (PAHO), approximately one in eight people in the world suffers from a mental health disorder. This condition is the main cause of years lived with disability (YLD), with one in six cases of YLD globally 1.
In Chile, the "ACHS-UC Mental Health Thermometer" study, whose ninth round was conducted in 2023, revealed that 13.4% of the people evaluated presented suspected mental health problems or issues, while 64% presented symptoms of depression and 55% reported anxious symptoms 2.
Users with mental health disorders access different levels of health services with the expectation of receiving care that alleviates or eradicates their condition 3. In this context, health care providers have the duty to provide accessible, timely, and quality care, without arbitrary discrimination, as stipulated in Article 2 of Law 20.584, which regulates the rights and responsibilities of individuals concerning actions related to health care 4. Likewise, the comprehensive family and community health care model reinforces the principle of person-centered care, promoting treatment based on dignity and respect 5.
Globally, there are gaps in mental health care coverage, which are exacerbated by the variable quality of care 6. Among the factors that prevent people with mental health disorders from accessing health care are poor quality of services, lack of knowledge about mental health, stigmatization, and discrimination 1.
The World Health Organization (WHO) notes 7 that stigma toward people with mental disorders is widespread in both society and health care systems around the world, leading to inefficient service delivery or difficulty accessing them. It notes, for example, that 71% of people with psychosis worldwide do not receive mental health services.
In light of this problem, PAHO 8 emphasizes that stereotypes, prejudices, and discriminatory behaviors toward people with mental health problems are common in health services. Therefore, in 2022, this organization promoted a global campaign aimed at curbing stigma and discrimination against these individuals.
At the national level, the Ministry of Health (MINSAL), through the National Mental Health Plan 2017-2025, defined stigma as a multidimensional phenomenon related to ignorance and fear of others. This phenomenon is reflected in social exclusion and mistreatment of people with these disorders, who are considered dangerous, unpredictable, and undesirable, as well as in a lack of opportunities for them 9,10. They emphasize that stigma constitutes a critical challenge for the integration of mental health into primary health care (PHC), highlighting that people with mental disorders may have more adverse experiences as service users compared to people without these diagnoses.
The sociocognitive theoretical model of mental stigma, proposed by Bandura, explains how the emotions, behaviors, and thoughts triggered by prejudice allow us to understand the determinants of stigma, guiding interventions at the individual and societal levels 11.
Given this scenario, it is essential to implement mental health policies and programs consistent with the community epidemiological paradigm, which requires a sustained effort and the active support of the entire community, including health system officials 12,13.
In this context, the present study aimed to evaluate the effectiveness of an anti-stigmatization intervention program targeting patients with mental disorders. The following objectives were set: To describe the level of stigmatization toward these patients by health professionals; to identify problem areas and factors contributing to stigma; to design an intervention program tailored to the identified needs and adapted to the context of the selected Health Center for the Prevention and Control of Mental Health (CESFAM, for its initials in Spanish), and to implement this program, incorporating training and awareness-raising activities for the facility's professionals.
Materials and Methods
A quantitative, analytical, pre-experimental, longitudinal study was conducted at a CESFAM in the Biobío region of Chile, part of the Talcahuano Health Service's PHC network. The intervened facility has a staff of 159 clinical and non-clinical staff members, with contracts valid until March 30, 2024, under permanent contract and fee-based modalities, excluding emergency service personnel.
The sample was drawn from the Human Resources payroll. The sample was selected using stratified random sampling, initially resulting in 61 participants. The selection criteria considered workers with more than one year of experience at the facility, whose duties involved maintaining direct contact with users and who attended at least one intervention workshop. On the other hand, workers with justified absenteeism during the questionnaire administration period and those who did not sign the informed consent form were excluded, leaving a final sample of 40 participants.
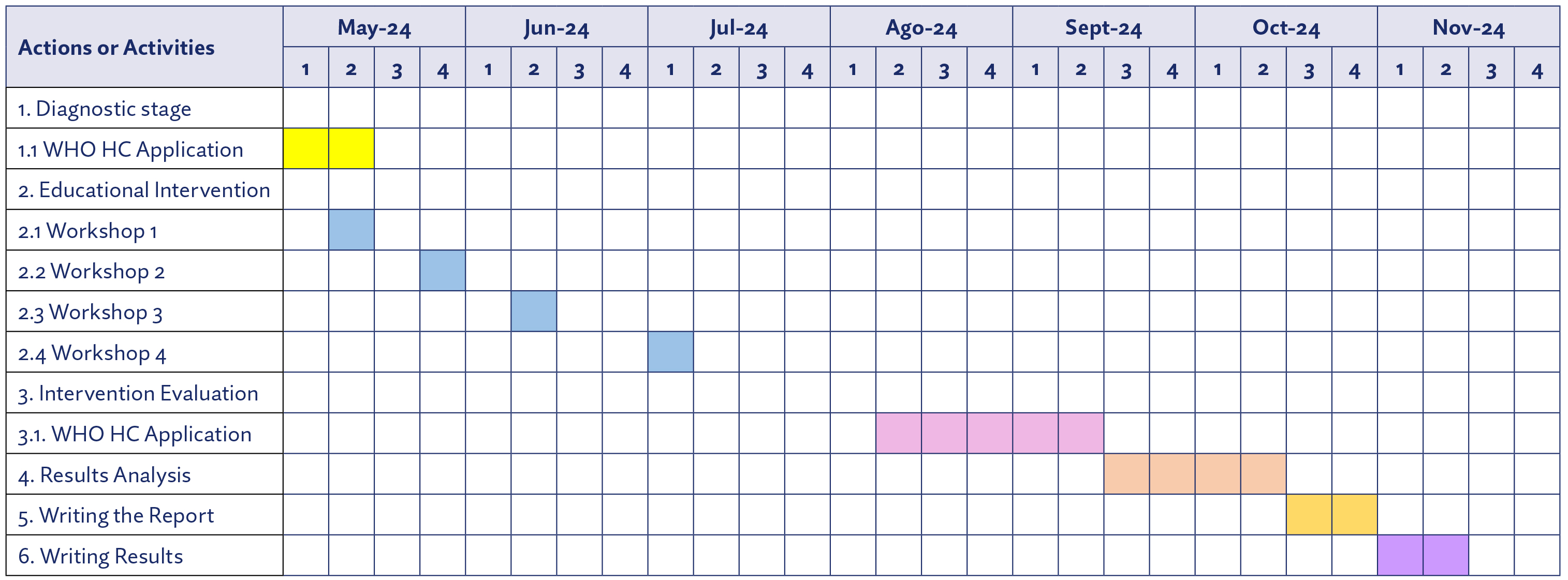
This intervention program aimed to reduce stigmatizing attitudes toward people with mental disorders by developing diagnostic, educational, and evaluative activities based on Bandura's social cognitive theory. The implementation of the anti-stigma program was implemented in four planned stages, which are detailed in Annex 2.
Diagnostic stage: This stage aimed to establish a baseline regarding the stigmatizing attitudes of the participants by applying the Opening Minds Stigma Scale for Health Care Providers (OMS-HC) questionnaire. Data collection took place in May 2024, allowing for the identification of key areas to address in the educational workshops.
Educational intervention stage: During this stage, four one-hour educational workshops were held, designed to address issues related to the stigmatization of people with mental disorders. These workshops ran from the last week of May to the first week of July 2024. The workshops were prepared and conducted with the support of a mental health professional and covered the following topics:
Workshop 1: A reflection workshop on mental health, focusing on stigma, discrimination, and their impact on people with mental disorders. This workshop sought to raise awareness among participants about how their attitudes can influence the care they provide to these patients.
Workshop 2: Self-esteem and self-perception, focusing on the relationship between personal perception and attitudes toward others.
Workshop 3: Psychological first aid for psychologically-unbalanced patients, which provided practical tools for dealing with crises.
Workshop 4: Proper treatment of people with mental disorders, which promoted skills to ensure respectful and dignified care.
Post-intervention questionnaire administration stage: In this stage, conducted between August and September 2024, the WHO-HC questionnaire was administered again, including an additional question on attendance at the educational workshops. This information allowed for the analysis of the intervention's effectiveness among participants who actively attended the sessions.
Results analysis: Data analysis was conducted between September and October 2024. This phase allowed for the evaluation of the intervention program's effectiveness, identifying changes in stigmatizing attitudes and establishing correlations between workshop participation and the results of the WHO-HC questionnaire.
The WHO-HC questionnaire (Annex 1), originally developed in Canada in 2012, assesses stigma towards people with mental disorders by health officials 14; Its reliability has been tested with a Cronbach's a index of 0.82 in 2012 and 0.76 in 2018, in Canada 15,16, and 0.74 in 2023, in Brazil 17. In Chile, a version was translated and validated by Sapag et al. 18 in 2019, with a Cronbach's a of 0.69; this version is structured around three dimensions: 1) attitudes toward people with mental illnesses; 2) disclosure and help-seeking; and 3) social distance. It is recommended that responses be analyzed in the context of these specific dimensions 18.
Later, in 2021, Gajardo et al. 19 also performed the translation and validation using the content validity index (CVI), which was considered acceptable with ranges between 0.51 and 0.99.
The WHO-HC questionnaire is a self-administered instrument consisting of 20 items with Likert-type response options on a scale of 1 to 5, where 1 means "completely disagree" and 5 means "completely agree." The scales indicate that a higher overall score indicates a more stigmatizing attitude, with 20 points being the lowest stigmatizing attitude and 100 points the highest. Questions 3, 8, 9, 10, 11, 15, and 19 are reverse-coded, with the lowest score assigned to "completely disagree" and the highest to "completely agree" 20.
To complete the sample characterization, a sociodemographic questionnaire was designed that included variables such as gender, age, status or profession, years of service, and the presence of a close relative with a mental health disorder.
Data collection: Data collection was conducted in two phases. The first was a pre-intervention diagnostic phase, which took place in May 2024, and the second was conducted post-intervention in August and September of the same year. Both phases used the WHO-HC questionnaire, in its validated and translated version for Chile, which was sent to study participants via email using a Google Forms link. For post-intervention data collection, an additional question about the anti-stigma workshops was incorporated into the questionnaire to assess participation.
Statistics: The statistical analysis included initial data tabulation in Microsoft® Excel®, followed by advanced processing using Jamovi® software, v. 2.3.28. Descriptive analyses of sociodemographic variables were performed, calculating frequencies and percentages. To compare the means of the total score of the instrument and its dimensions, the Student t test was applied for paired samples, with the exception of the disclosure dimension. The latter, as it did not present a normal distribution, was analyzed using the Wilcoxon W test. Additionally, one-way analysis of variance (ANOVA), Games-Howell post-hoc tests, and Spearman's Rho were used to evaluate the correlation between variables and identify groups with significant differences.
Ethical Considerations: To guarantee the anonymity of the participants and the appropriate use of the information, in accordance with the provisions of Chilean Law 19.628 on the Protection of Private Life 21, the prior, free and informed consent of those involved was obtained. In addition, it was verified that this project did not entail risks of destruction, death or serious and lasting bodily injury to the participants. Therefore, approval was requested from the scientific ethics committee of the affiliated university, in compliance with Article 10 of Law 20.120 22, which was granted through opinion No. 2024-02.
Results
The most relevant results from the application of the WHO-HC questionnaire in the pre- and post-intervention stages are presented below and complemented by an analysis of the participants' sociodemographic variables. These data allowed us to observe the changes and dynamics in responses before and after the intervention, allowing us to evaluate the program's impact, contextualize the stigma phenomenon and explore possible relationships between participants' characteristics and their respective responses.
Regarding the sociodemographic data of the sample, composed of 40 people, it was found that the predominant gender was female (72.5%); males accounted for 27.5%. Regarding age distribution, the 30-39 age group was the most represented (45%), followed by the 40-49 age group (25.5%), and the 50-59 age group (20%). The most prominent group was professionals, representing 57.5% of the total, followed by technicians (32.5%) and administrative staff (10%). Regarding years of service, the most prominent group was 8-12 years (32.5%), followed by 4-7 years (20%), and 21-35 years (17.5%). Regarding the item "presence of a close relative with a mental illness," an increase in affirmative responses was observed in the post-intervention questionnaire. The number of participants who reported having relatives diagnosed with a mental disorder increased from 19 at pre-intervention to 26 at post-intervention, which translates, in percentage terms, into a variation ranging from 47.5% to 65%, respectively. Table 1 shows a more detailed analysis of this question in the pre-intervention stage, comparing the "yes" and "no" responses for both the total questionnaire score and each of its dimensions. For the total questionnaire, the means are similar for "yes" and "no," 44.6% and 47.6%, respectively.
Table 1 Presence of a Close Relative with a Mental Health Illness before the Intervention
Yes |
No |
|||||
|---|---|---|---|---|---|---|
Variables |
M |
SD |
M |
SD |
t of |
p |
Questionnaire Total |
44,6 |
8,98 |
47,6 |
7,58 |
-1122<7 |
0,269 |
Disclosure and help-seeking |
7,89 |
3,23 |
8,05 |
2,40 |
-0.171 |
0,865 |
Social Distance |
9,42 |
2,76 |
10,7 |
3,09 |
-1340 |
0,188 |
Attitudes toward people with mental illness |
12,8 |
3,20 |
13,9 |
3,19 |
-1050 |
0,300 |
Source: Prepared by the authors.
Note: M = mean, SD = standard deviation, p = p-value
Table 2 presents a descriptive analysis of the entire questionnaire and each of its dimensions in the pre- and post-intervention stages. The results show that the mean for the entire instrument remained constant at 46.2 in both the pre- and post-intervention stages. However, a slight variation in the SD was observed, being ±8.30 in the pre-intervention and ±9.43 in the post-intervention. The statistical analysis yielded a p-value of 0.982. Regarding the dimension "attitude toward people with mental illnesses," this showed a slight variation in means, from 13.4 to 14.1, with an SD of ±3.20 and 3.65, respectively, and a p-value of 0.443. Finally, in the "disclosure and help-seeking" dimension, a slight increase in the mean was observed, from 7.97 to 8.32, with a SD variation of ±2.67 to 2.96 and a p-value of 0.544.
Table 2 Questionnaire Totals and Comparison of Means for Each Dimension
Pre-Intervention |
Post Intervention |
||||||
|---|---|---|---|---|---|---|---|
Variables |
M |
SD |
M |
SD |
Test |
Statistic |
P |
Pre-intervention social distancing |
10,1 |
3,10 |
10,2 |
3,20 |
t of Student |
-0,1575 |
0,876 |
Attitudes toward people with mental illness pre-intervention |
13,4 |
3,20 |
14,1 |
3,65 |
t of Student |
-0,7759 |
0,443 |
Pre-intervention disclosure |
7,97 |
2,79 |
8,32 |
2,79 |
W of Wilcoxon |
329 |
0,544 |
Source: Prepared by the authors.
Note: M = mean, SD = standard deviation, p = p-value. Attitudes toward people with mental illness: Maximum score of 30.
Disclosure and help-seeking: Maximum score of 20. Social distancing: Maximum score of 25.
An analysis was performed to associate the variables "statuses" and the "social distance" dimension in the pre-intervention stage, since no statistically significant differences were found between the pre- and post-intervention stages. The one-way ANOVA showed a p-value of 0.010, indicating significant differences. The descriptive analysis revealed that the administrative group obtained a mean of 13.5 points with an SD ± 1.9, being the highest score. The Games-Howell post-hoc test showed that the administrative group had a mean difference of -4.46 compared to the professionals, with a p-value of 0.020, as shown in Table 3.
Table 3 Games-Howell Post-Hoc Test between Groups and Pre-Intervention Social Distance
Class |
Social Distance |
|||||
|---|---|---|---|---|---|---|
Class |
Professional |
Trades |
Management |
M |
SD |
|
Professionals |
Difference of means |
-- |
-1,80 |
-4,46 |
9,04 |
2,85 |
P |
-- |
0,135 |
0,020 |
|||
Trades |
Difference of means |
-- |
-2,65 |
10,8 |
2,48 |
|
P |
-- |
0,135 |
||||
Management |
Difference of means |
-- |
13,5 |
1,91 |
||
P |
-- |
|||||
Source: Prepared by the authors.
Note: M = mean, SD = standard deviation, p = p-value. Attitudes toward people with mental illness: Maximum score of 30.
Disclosure and help-seeking: Maximum score of 20. Social distancing: Maximum score of 25.
Table 4 presents the relationship between years of service and attitudes toward people with mental illnesses before the intervention. Workers between the ages of 21 and 35 years had the highest mean score compared to the other groups, with an SD of ±3.35. The age group with the lowest mean score was the 1-3 years age group, with a mean of 10.2 and an SD of ±1.72.
Table 4 Attitudes toward People with Mental Illnesses and Years of Service
Pre-Intervention Results |
||
|---|---|---|
Years of Service |
M |
SD |
31 to 35 years |
14,0 |
NaN |
21 to 35 years |
14,3 |
3,35 |
13 to 20 years |
13,4 |
1,95 |
8 to 12 years |
14,2 |
2,71 |
4 to 7 years |
13,6 |
4,41 |
1 to 3 years |
10,2 |
1,72 |
Source: Prepared by the authors.
Note: M = mean, SD = standard deviation, NaN = no standard deviation.
Continuing with the results, a correlation was evident between the dimension of attitudes toward people with mental illnesses and years of service in the pre-intervention stage. Spearman's rho coefficient was 0.345, with a p-value of 0.029.
Finally, a comparison is presented between the age range and the dimension "attitudes toward people with mental illnesses" in the pre-intervention phase. For this comparison, the one-way ANOVA test showed a p-value of 0.003, indicating significant differences. Further descriptive analysis revealed that the 20- to 29-year-old group obtained significantly different scores compared to other age groups, with a mean of 10.0 points and a SD of ±1.00, representing the lowest score recorded. The Games-Howell post-hoc test revealed significant negative differences between this group and the other age groups, with p-values of 0.036, 0.005, and 0.042, respectively, as detailed in Table 5.
Table 5 Games-Howell Post-Hoc Test between Age Range and Attitudes toward People with Mental Illnesses Pre-Intervention
Age |
Attitudes toward people with mental |
||
|---|---|---|---|
M |
SD |
||
20 to 29 years |
Difference of means |
10,0 |
1,00 |
30 to 39 years |
Difference of means |
13,2 |
3,52 |
40 to 49 years |
Difference of means |
14,8 |
3,06 |
50 to 59 years |
Difference of means |
13,3 |
2,25 |
Source: Prepared by the authors.
Note: M = mean, SD = standard deviation, p = p-value.
Attitudes toward people with mental illness: Maximum score 30 points; Disclosure and help seeking: Maximum score 20 points; Social Distance: Maximum score 25 points.
Discussion
Evaluating the impact of an intervention aimed at reducing stigma toward people with mental disorders requires considering the interaction of individual, organizational, and intervention design factors. In this study, no statistically significant differences were observed in the WHO-HC questionnaire scores between the pre- and post-intervention stages, with an overall mean of 46.2 points (p = 0.982). This result may be related to the intensity and duration of the intervention, partial workshop attendance, and the working conditions of the healthcare team, factors that have been highlighted in the literature as determinants of success in anti-stigma interventions 20,23.
Similar results have been reported by Mittal et al. 24 and Al-madani et al. 25, in which educational interventions for healthcare professionals and students also failed to generate statistically significant changes. Sherwood 23 highlights that brief programs, focusing exclusively on theoretical content, often have a limited effect when they do not incorporate experiential components or direct contact with diagnosed individuals. This assertion finds support in the review by Arroyo et al. 26, who recommend good practices such as the testimony of people with lived experience and participatory strategies to achieve real change in the attitudes of healthcare personnel.
Although no overall quantitative changes were observed, an interesting finding was the increase from 47% to 65% in the reporting of close relatives diagnosed with a mental disorder. Although this change did not translate into differences in stigmatization levels, it could be interpreted as an indicator of greater awareness and willingness to recognize these conditions in one's personal environment. Studies such as those by Gajardo et al. 19 and Sapag et al. 10 have indicated that closeness to diagnosed individuals can reduce prejudice, although this study did not find a significant effect. In contrast, Torres et al. 28 reported a significant difference between those who did and did not have a relative with a mental illness, which contradicts the findings of the present study and underscores the importance of context.
Regarding baseline levels of stigmatization, the observed values are in the moderate-to-low range, consistent with research conducted in Hungary, the United States, and Portugal 29,30, and with the averages reported by 20 in Chilean clinical settings. However, these values were higher than those reported by Torres et al. 28, who obtained an average of 35 points among primary health care professionals. This discrepancy could be related to differences in participant profiles, the institutional setting, or the degree of prior exposure to mental health programs.
The analysis by dimensions of the WHO-HC questionnaire also showed no significant changes after the intervention. Scores on "Social Distance," "Attitudes toward People with Mental Illness," and "Disclosure and Help-Seeking" were similar to those reported in previous studies 20,30. However, as Hsia et al. 30 indicate, these dimensions may require differentiated approaches beyond traditional educational approaches.
Since no changes were observed after the intervention, a more in-depth analysis of the pre-intervention data was conducted. The analysis showed that the younger group of workers (20-29 years old) presented significantly lower levels of stigmatization compared to the older groups (p = 0.003), suggesting that younger generations may be more open to mental health. This result contrasts with the studies by Sapag and Velasco 20,31, who found lower levels of stigmatization in workers over 55 years of age. These differences could be explained by cultural, generational, or educational factors.
Likewise, significant differences were identified between levels, with administrative staff reporting the highest scores on the "Social Distance" dimension (p = 0.020). This finding is consistent with that observed by Sapag and Velasco 20,31, as the administrative staff showed higher levels of stigma compared to clinical staff, reinforcing the need to include all levels of the healthcare team in continuing education programs in mental health. Another relevant finding was the positive correlation between years of service and stigmatizing attitudes (p = 0.345; p = 0.029). The longer the service tenure, the more likely it was for higher stigma scores, particularly in the "Attitudes toward People with Mental Illness" dimension. This result is consistent with the study by Zamorano et al. 32, who found that professionals with more experience reported higher levels of stigma.
Stigmatization symptoms are also associated with depersonalization symptoms. However, this relationship is not unequivocal; Román 33, for example, found that a longer professional career was associated with greater empathy towards users with mental disorders, which shows the need to delve deeper into the mediating factors of this relationship.
Although this study did not demonstrate a significant reduction in stigma, it does contribute to highlighting the complexity of the phenomenon in primary care and to recognizing the need to strengthen educational programs with structured, experiential, and sustained components. Research such as that by Upegui et al. 34 and Gómez et al. (35) has shown that prolonged interventions, which include reflective elements, contact with people with lived experience, and follow-up, significantly reduce stigma.
In line with the recommendations of Arroyo et al. 27, future strategies should combine technical training, direct contact, and active participation, while also strengthening institutional support as a protective factor against discriminatory attitudes. This study provides a useful empirical basis for planning more comprehensive and locally tailored programs and underscores that generating real transformation requires more than single workshops but requires systematic, collaborative, and sustained efforts.
Conclusion
This study evaluated the impact of an educational intervention aimed at reducing stigma toward people with mental disorders in primary care. Although no statistically significant changes in overall stigma levels were observed between pre- and post-intervention measurements, the results offer useful information for understanding implementation challenges in real-world settings and provide key guidance for strengthening future training strategies.
The study also identified relevant factors associated with stigma, such as age, occupational status, and years of service. Lower levels were observed among younger professionals, and higher scores were observed among administrative staff and workers with more seniority. There was also an increase in the number of participants who reported having a mental health diagnosis after the intervention, which could reflect greater openness or awareness on the topic.
Overall, the findings underscore the importance of moving toward more comprehensive, experiential, and sustained educational interventions that have institutional support and consider the characteristics of the healthcare team. Strengthening these programs is key to fostering more empathetic, inclusive, and patient-centered care environments.
Practical Implications
The results highlight the need to optimize anti-stigma strategies, incorporating more effective approaches tailored to professionals and supported by institutions to ensure their impact and sustainability.
Limitations
The main limitations of the research were:
Limited participation and attendance: Low attendance at the workshops affected the representation of the results and the potential reach of the program.
Perceived judgment: Some participants feared being identified as stigmatizers, which may have influenced their willingness to actively participate or express their true attitudes during the intervention.
Workload and limited time: The health workers' busy schedules, combined with their work responsibilities, limited their availability to attend sessions, which affected both participation and the effectiveness of the anti-stigma program.
Suggestions
For future research, the following is suggested:
Improve workshop participation through strategies such as incentives and schedule adjustments, or workshops at different times or on different dates to make them more accessible to all employees.
Implement a survey or interview system before and after each workshop to collect feedback and adjust session design based on the needs of the participants.
Raise awareness among the administration about the importance of maintaining anti-stigma programs for people with mental disorders, ensuring continuity over time and institutional support.
Declaration of interests:
The authors declare there are no competing, financial, or personal interests that could affect the development, results, or interpretation of this project.
Financial support
This research did not receive any external funding or grants, nor did it receive financial support through internal university projects.
References
1. Organización Panamericana de la Salud. Informe mundial sobre la salud mental: Transformar la salud mental para todos [Internet]. Washington D.C: OPS; 2023. https://doi.org/10.37774/9789275327715
2. Casali R, Maldonado A, Riquelme M. Novena ronda del Termómetro de la Salud Mental Achs-UC. ACHS [Internet]; 2024. https://www.achs.cl/centro-de-noticias/noticia/2024/novenaronda-del-term%C3%B3metro-de-la-salud-mental-achs-uc
3. Pérez LA, Mantilla MI, Munoz E. Perspectivas de la salud mental en el escenario laboral: anatomía de un debate académico. Rev Cuba Salud Publica [Internet]. 2021;47(4). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-34662021000400017
4. Ministerio de Salud, Subsecretaría de Salud Pública. Ley 20.584, que regula los derechos y deberes que tienen las personas en relación con acciones vinculadas a su atención en salud; 24 de abril de 2012. https://www.leychile.cl/Navegar?idNorma=1039348
5. Subsecretaría de Redes Asistenciales-Minsal. Orientaciones para la Planificación y Programación en Red 2024; 2023. https://www.minsal.cl/orientaciones-para-la-planificacion-y-programacion-en-red/
6. Gomero G. Influencia de las barreras en salud en la reducción de brechas en el servicio de medicina, Centro de Salud Huaraz, Tesis de maestría en Gestión Pública en Internet. Lima: Universidad César Vallejo; 2023. https://repositorio.ucv.edu.pe/bitstream/handle/20.500.12692/123484/Gomez_AGE-SD.pdf
7. World Health Organization (WHO). La OMS subraya la urgencia de transformar la salud mental y los cuidados conexos; 2022. https://www.who.int/es/news/item/17-06-2022-who-highlights-urgent-need-to-transform-mental-health-and-mentalhealth-care
8. PAHO/WHO | Pan American Health Organization [Internet]. La OPS lanza nueva campana para frenar el estigma hacia las personas con problemas de salud mental; 7 de octubre de 2022. https://www.paho.org/es/noticias/7-10-2022-ops-lanza-nueva-campana-para-frenar-estigma-hacia-personas-con-problemas-salud
9. MINSAL. Plan Nacional de Salud Mental 2017-2025; 7 de diciembre de 2017. https://www.minsal.cl/wp-content/uploads/2017/12/PDF-PLAN-NACIONAL-SALUD-MENTAL-2017-A-2025.-7-dic-2017.pdf
10. Sapag JC, Traub C, Velasco PR, Arratia T, Alvarado R, Aracena M, et al. Reducing Stigma toward Mental Illness and Substance Use Issues in Primary Health Care in Chile; Protocol of Cluster Controlled Trial Study. Front Psychiatry [Internet]. 2022;13. https://doi.org/10.3389/fpsyt.2022.1083042
11. De la Fuente J, Kauffman DF, Boruchovitch E. Past, Present and Future Contributions from the Social Cognitive Theory (Albert Bandura). Front Psychol. 2023;14:e1258249. https://doi.org/10.3389/fpsyg.2023.1258249
12. Valderrama-Núnez C, Zolezzi-Gorziglia R. Intersectorialidad y reducción del estigma en salud mental: la necesidad de avanzar hacia una descolonización de la institucionalidad, desde una perspectiva intercultural. Saude Soc [Internet]. 2021;30(4). https://doi.org/10.1590/s0104-12902021200973
13. Zabaleta-González R, Lezcano-Barbero F, Perea-Bartolomé MV. Análisis de los Programas educativos sobre alfabetización en salud mental. Revisión documental. Rev Complut Educ [Internet]. 2021;33(1):57-69. https://doi.org/10.5209/rced.73696
14. Stuart H, Dobson K. Stigma of Mental Illness: Models and Methods of Stigma Reduction [Internet]. Oxford University Press, Incorporated; 2021. https://doi.org/10.1093/med/9780197572597.001.0001
15. Kassam A, Papish A, Modgill G, Patten S. The Development and Psychometric Properties of a New Scale to Measure Mental Illness Related Stigma by Health Care Providers: The Opening minds Scale for Health Care Providers (OMS-HC). BMC Psychiatry [Internet]. 2012;12(1). https://doi.org/10.1186/1471-244X-12-62
16. Van der Maas M, Stuart H, Patten SB, Lentinello EK, Bobbili SJ, Mann RE, et al. Examining the Application of the Opening Minds Survey in the Community Health Centre Setting. Can J Psychiatry [Internet]. 2017;63(1):30-6. https://doi.org/10.1177/0706743717719079
17. Carrara BS, Sanches M, Bobbili SJ, de Godoy Costa S, de Sousa ÁF, de Souza J, et al. Validation of the Opening Minds Scale for Health Care Providers (OMS-HC): Factor Structure and Psychometric Properties of the Brazilian Version. Healthcare [Internet]. 2023;11(7):1049. https://doi.org/10.3390/healthcare11071049
18. Sapag JC, Klabunde R, Villarroel L, Velasco PR, Álvarez C, Parra C, et al. Validation of the Opening Minds Scale and Ptterns of Stigma in Chilean Primary Health Care. PLOS ONE [Internet]. 2019;14(9):e0221825. https://doi.org/10.1371/journal.pone.0221825
19. Gajardo JJ, Espinosa TF, Munoz EI, Goycolea MR, Valdebenito A, Oyarzún SM, et al. Traducción y análisis de validez de contenido del instrumento Opening Minds Scale for Healthcare Practitioners (OMS-HC) para la evaluación del estigma hacia la enfermedad mental en profesionales de la salud en Chile. Rev Chil Neuro Psiquiatr [Internet]. 2021;59(2):91-101. https://doi.org/10.4067/s0717-92272021000200091
20. Gajardo J, Espinosa F, Goycolea R, Oyarzún M, Munoz I, Valdebenito A, et al. Estigma hacia personas con enfermedad mental en estudiantes y profesores de terapia ocupacional. Cad Bras Ter Ocupacional [Internet]. 2022;30. https://doi.org/10.1590/2526-8910.ctoao24103145
21. Ministerio Secretaría General de la Presidencia. Ley 19628, Sobre protección de la vida privada, 18 de agosto de 1999; 28 de agosto de 1999 https://www.leychile.cl/Navegar?idNorma=141599
22. Ministerio de Salud, Subsecretaría de Salud Pública. Ley 20120, Sobre la investigación científica en el ser humano, su genoma, y prohibe la clonación humana, 7 de septiembre de 2006; 22 de septiembre 2006. https://www.leychile.cl/Navegar?idNorma=253478
23. Sherwood DA. Healthcare Curriculum Influences on Stigma towards Mental Illness: Core Psuchiatric Course Impact on Pharmacy, Nursing and Social Work Student Attitudes. Curr Pharm Teach Learn [Internet]. 2019;11(2):198-203. https://doi.org/10.1016/j.cptl.2018.11.001
24. Mittal D, Owen RR, Ounpraseuth S, Chekuri L, Drummond KL, Jennings MB, et al. Targeting Stigma of Mental Illness among Primary Care Providers: Findings from a Pilot Feasibility Study. Psychiatry Res [Internet]. 2020;284:112641. https://doi.org/10.1016/j.psychres.2019.112641
25. Almadani AH, AbuDujain NM, Alzahrani A, AlJaffer MA. Stigma toward Mental Illness among Saudi Medical Students. J Nerv Ment Dis [Internet]. 2023;211(2):157-162. https://doi.org/10.1097/NMD.0000000000001582
26. Arroyo Cifuentes JL, Díaz Mandado O, García de Mateos Granda AM, Gil Sanz D, González Blanco M, González Rueda R, et al. Guía de buenas prácticas para la realización de acciones de lucha contra el estigma. Inf Psiquiatr [Internet]. 2023;(252):9-26. https://www.informacionespsiquiatricas.com/storage/article/pdfs/7b1b1add5b2616fcf64197e04bc57860.pdf
27. Torres IN, Pereira HP, Moreira MB, Marina S, Ricou M. Prevalence of stigma towards mental illness among Portuguese healthcare professionals: a descriptive and comparative study. Front Psychiatry [Internet]. 2024;15. https://doi.org/10.3389/fpsyt.2024.1425301
28. Őri D, Szocsics P, Molnár T, Ralovich FV, Huszár Z, Bene Á, et al. Stigma towards mental illness and help-seeking behaviors among adult and child psychiatrists in Hungary: A cross-sectional study. PLoS ONE [Internet]. 2022;17(6):e0269802. https://doi.org/10.1371/journal.pone.0269802
29. Hsia SL, Brooks J, Yao E, Gruenberg K, Finley P. Impact of an auditory hallucination simulation coupled with a speaker diagnosed with schizophrenia on mental illness stigma in pharmacy students. Curr Pharm Teach Learn [Internet]. 2022;14(11):1397-1403. https://doi.org/10.1016/j.cptl.2022.09.022
30. Sapag JC, Velasco PR. Estigma hacia los trastornos mentales y adicciones: estudio en la atención primaria de Chile. Atención Primaria [Internet]. 2020;52(5):361-3. https://doi.org/10.1016/j.aprim.2019.07.014
31. Zamorano S, González-Sanguino C, Fernández-Jiménez E, Munoz M. A Burnt-Out Health: Stigma towards Mental Health Problems as a Predictor of Burnout in a Sample of Community Social Healthcare Professionals. Behav Sci [Internet]. 2024;14(9):812. https://doi.org/10.3390/bs14090812
32. Román D. Empatía, burnout y actitudes hacia los pacientes con trastorno mental: un estudio en el ámbito de la enfermería, [Tesis doctoral]. Cádiz: Universidad de Cádiz; 2022. http://hdl.handle.net/10498/28894
33. Sukhera J, Miller K, Scerbo C, Milne A, Lim R, Watling C. Implicit Stigma Recognition and Management for Health Professionals. Acad Psychiatry [Internet]. 2019;44(1):59-63. https://doi.org/10.1007/s40596-019-01133-8
34. Martin A, Chilton J, Paasche C, Nabatkhorian N, Gortler H, Cohenmehr E, et al. Shared Living Experiences by Physicians have a Positive Impact on Mental Health Attitudes and Stigma among Medical Students: A Mixed-Methods Study. J Med Educ Curric Dev [Internet]. 2020;7:238212052096807. https://doi.org/10.1177/2382120520968072
ANNEXES
Annex 1. Opening Minds Stigma for Healthcare Providers (OMS-HC) Questionnaire
1. Identify your gender
• Femenine
• Masculine
• Other
2. Age (Years)__________________________
3. Class
• Professionals
• Trades
• Management
• Auxiliaries
• Other
4. Indicate your current profession__________________
5. Indicate the years of service completed in the health area__________________
6. Do you have a loved one diagnosed with a mental health disorder?
• Yes
• No
Open Minds Scale for Health Professionals (WHO-HC)
Translated version in Chile (Gajardo et al., 2021)
Statement |
Completely |
Disagree |
Neither agree |
Agree |
Completely |
|---|---|---|---|---|---|
1. I feel more comfortable caring for a person with a physical illness than for a person with a mental illness. |
|||||
2. If a person with a mental illness complains of physical symptoms (e.g. nausea, back pain, headache), I would probably attribute it to their mental illness. |
|||||
3. If a coworker told me that he or she had a mental illness under control, I would remain willing to work with him or her. |
|||||
4. If I were being treated for a mental illness, I wouldn't tell any of my coworkers. |
|||||
5. I would be more willing to seek help for a mental illness if the health professional treating me was not connected to my workplace. |
|||||
6. I would consider myself a weak person if I had a mental illness and couldn't solve it on my own. |
|||||
7. I would be reluctant to seek help if I had a mental illness |
|||||
8. Employers should hire a person who has a mental illness under control, if he or she is the best candidate for the job. |
|||||
9. If I knew that a doctor had been treated for a mental illness, I would still see him or her. |
|||||
10. If I had a mental illness I would tell my friends. |
|||||
11. Health professionals have a responsibility to convey to people with a mental illness that their life will be better. |
|||||
12. A pesar de mis convicciones profesionales, tengo reacciones negativas hacia personas que tienen una enfermedad mental |
|||||
13. I can't do much to help people who have a mental illness. |
|||||
14. More tan half of the people with mental illness do not make enough efforts to get better. |
|||||
15. People with mental illness rarely pose a risk to the public. |
|||||
16. The best treatment for mental illness is medication |
|||||
17. I would not like that a person with a mental illness worked with children even he/she had it under control. |
|||||
18. Health professionals do not need to be advocates of people with a mental illness. |
|||||
19. I would not mind if a person with a mental illness was my neighbor. |
|||||
20. It is difficult for me to feel empathy for what a person with mental illness experiences. |
Annex 2 Gantt Chart Intervention Project: