
|
|
ARTICLE

Catalina Constanza Sepúlveda Rivas 1
Nelson Felipe Medina Leal 2
Edith Rivas Riveros 3
Maggie Campillay Campily 4
1 Universidad Santo Tomás, Chile
![]() 0000-0002-5256-2270
0000-0002-5256-2270
![]() catalinasepulvedan@santotomas.cl
catalinasepulvedan@santotomas.cl
2 Universidad Santo Tomás, Chile
![]() 0000-0002-8357-6245
0000-0002-8357-6245
![]() nmedina3@santotomas.cl
nmedina3@santotomas.cl
3 Universidad de La Frontera, Chile
![]() 0000-0002-9852-4534
0000-0002-9852-4534
![]() edith.rivas@ufrontera.cl
edith.rivas@ufrontera.cl
4 Universidad de Atacama, Chile
![]() 0000-0002-4054-1595
0000-0002-4054-1595
![]() maggie.campillay@uda.cl
maggie.campillay@uda.cl
Theme: Health, well-being, and quality of life promotion
Contribution to the field: This study contributes to disciplinary knowledge by integrating the ABCD model into the care of chronic diseases such as hypertension and type II diabetes, highlighting the importance of community networks and collective action in improving health. By applying a salutogenic approach, it emphasizes the value of community resources in health promotion, addressing gaps in access and strengthening the active participation of communities. This approach contributes to the development of community intervention models in nursing, promoting inter-institutional collaboration and mutual support.
Received: 16/01/2025
Sent to peers: 01/04/2025
Approved by peers: 23/04/2025
Accepted: 29/04/2025
Para citar este artículo / To reference this article / Para citar este artigo Sepúlveda C, Medina N, Rivas E, Campillay M. Gaps in the Salutogenesis ff Hypertension and Type II Diabetes ign Chile. Aquichan. 2025;25(3):e2532. DOI: https://doi.org/10.5294/aqui.2025.25.3.2
Abstract
Introduction: This study presents the research on health improvement in people with chronic cardiovascular diseases, such as hypertension and type II diabetes, using a salutogenic approach. Unlike other studies, it incorporates the asset-based community development (ABCD) model, which prioritizes community resources and collective collaboration, rather than focusing solely on conventional medical care.
Objective: To identify gaps, assets, and challenges in the care of these diseases from the perspective of patients and healthcare professionals.
Materials and Methods: A descriptive qualitative study was conducted with 12 patients from community associations who had hypertension and/or type II diabetes, and 8 healthcare professionals selected by purposive sampling. Data were collected through semi-structured interviews and analyzed using the ABCD model, which promotes social networking and collective action. Methodological rigor was ensured through data triangulation and specialist validation.
Results: The data analysis enabled the creation of a map of community assets, identifying key actors and their interactions. The ABCD model was used to understand how community resources influence care and the capacity for collective action. Among the challenges encountered, the lack of collaboration between patients and healthcare professionals, misinformation regarding care options, and inequality in access to healthcare services, particularly in rural areas, stand out.
Conclusions: The study highlights the importance of the ABCD model in strengthening community networks and improving care processes, especially in rural and neglected communities.
Keywords (Source: DeCS): Health promotion; community participation; hypertension; type 2 Diabetes Mellitus; community networks
Resumen
Introducción: Este estudio investiga la mejoría de la salud en personas con enfermedades cardiovasculares crónicas, como hipertensión y diabetes tipo II mediante un enfoque salutogénico. A diferencia de otros estudios, incorpora el modelo de desarrollo comunitario basado en activos (ABCD), que prioriza los recursos comunitarios y la colaboración colectiva, en lugar de enfocarse únicamente en la atención médica convencional.
Objetivo: Identificar las brechas, activos y desafíos en el cuidado de estas enfermedades desde la perspectiva de pacientes y profesionales de salud.
Métodos: Se realizó un estudio cualitativo descriptivo con 12 pacientes de asociaciones comunitarias con hipertensión y/o diabetes tipo II, y 8 profesionales de salud seleccionados por muestreo intencional. Los datos se recopilaron mediante entrevistas semiestructuradas y se analizaron usando el modelo ABCD, que promueve la creación de redes sociales y la acción colectiva. El rigor metodológico se garantizó mediante triangulación de datos y validación por expertos.
Resultados: El análisis de los datos permitió la construcción de un mapa de activos comunitarios, identificando actores clave y sus interacciones. El modelo ABCD se utilizó para entender cómo los recursos comunitarios influyen en el cuidado y la capacidad de acción colectiva. Entre los desafíos encontrados, destacan la falta de colaboración entre pacientes y profesionales de salud, la desinformación sobre opciones de cuidado y la desigualdad en el acceso a servicios de salud, especialmente en zonas rurales.
Conclusiones: El estudio resalta la importancia del modelo ABCD para fortalecer las redes comunitarias y mejorar los procesos de atención, especialmente en comunidades rurales y desatendidas.
Palabras clave (Fuente: DeCS): Promoción de la salud; participación de la comunidad; hipertensión; diabetes tipo ii; redes comunitarias
Resumo
Introdução: Este estudo investiga a melhoria da saúde em pessoas com doenças cardiovasculares crônicas, como hipertensão e diabetes tipo II, por meio de uma abordagem salutogênica. Ao contrário de outros estudos, ele incorpora o modelo de desenvolvimento comunitário baseado em ativos (ABCD), que prioriza os recursos da comunidade e a colaboração coletiva, em vez de focar somente no atendimento médico convencional.
Objetivo: Identificar as lacunas, os ativos e os desafios do cuidado dessas doenças na perspectiva de pacientes e profissionais de saúde.
Materiais e métodos: Foi realizado um estudo qualitativo descritivo com 12 pacientes de associações comunitárias com hipertensão e/ou diabetes tipo II e 8 profissionais de saúde selecionados por amostragem intencional. Os dados foram coletados por meio de entrevistas semiestruturadas e analisados segundo o modelo ABCD, que promove a criação de redes sociais e ações coletivas. O rigor metodológico foi garantido por meio da triangulação e validação dos dados por especialistas.
Resultados: A análise dos dados permitiu elaborar um mapa dos ativos comunitários, identificando os principais atores e suas interações. O modelo ABCD foi utilizado para entender como os recursos da comunidade influenciam o cuidado e a capacidade de ação coletiva. Entre os desafios encontrados, destacam-se a falta de colaboração entre pacientes e profissionais de saúde, a desinformação sobre as opções de atendimento e a desigualdade no acesso aos serviços de saúde, especialmente nas áreas rurais.
Conclusões: O estudo ressalta a importância do modelo ABCD para fortalecer as redes comunitárias e melhorar os processos de atendimento, especialmente em comunidades rurais e carentes.
Palavras-chave (Fonte: DeCS): Promoção da saúde; participação comunitária; hipertensão; diabetes tipo II; redes comunitárias
Introduction
Cardiovascular diseases (CVDs) remain the leading cause of mortality and the burden of disease and disability in the Americas. In 2019, two million people died from CVDs 1. The situation is similar in Chile, where CVDs were the leading cause of death in 2017, accounting for 27.9 % of all deaths 2.
The World Health Organization (WHO) has published its first report on the devastating global effects of high blood pressure (HBP). According to the report, approximately four out of five people with HBP do not receive adequate treatment. However, if countries manage to expand coverage, 76 million deaths could be prevented between 2023 and 2050 3. Risk factors include high sodium intake, low fruit and vegetable intake, harmful use of alcohol, and physical inactivity, as well as high blood pressure combined with tobacco use, obesity, diabetes, or high cholesterol, which increases the risk of CVDs 4.
Data from the WHO show that 46 °% of adults with hypertension are unaware that they have this condition. Hypertension is diagnosed and treated in less than half of all adults who have it (only 42 %). Furthermore, only one in five adults with hypertension (21 %) has the condition under control, despite it being one of the leading causes of premature death worldwide 5. In turn, evidence suggests that HBP can reduce people's quality of life due to multiple complications in target organs and the side effects of antihypertensive medications. It is important to control it to significantly reduce the risk of complications and improve people's quality of life 6.
Meanwhile, diabetes mellitus (DM) is a chronic disease that, if left uncontrolled, mainly causes hyperglycemia, which over time seriously damages essential organs and systems 7, primarily leading to blindness, kidney failure, heart attacks, strokes, and lower limb amputations. Poorly controlled diabetes increases the risk of these complications and premature mortality 8. A study reveals that, in the Americas, 112 million adults (13 % of the adult population) live with diabetes, which is almost four times the number of adults living with diabetes in 1990 (30 million, 7 % of the adult population). The largest increases occurred in low-middle-income countries, where diabetes rates have skyrocketed while access to treatment remains limited 9.
In addition, quality of life is affected by the emotional component generated by dietary and physical restrictions, impacting aspects such as emotional well-being, as strict diets can generate feelings of anger, depression, and frustration 10.
A review based on the following research question: "What is the relationship between salutogenesis, sense of coherence, and cardiovascular health in adults?" found that the salutogenic model, with its positive approach to health, promotes the necessary motivation for people to face the challenges that arise throughout life 11. This led to the development of the salutogenic theory, which highlights the foundational elements of health and well-being, with a primary focus on factors that actively promote health 12.
Thus, Antonovsky's salutogenic theory proposes a paradigm shift from the pathogenic approach. While the latter focuses on the negative risk factors that explain why people become ill, the salutogenic approach focuses on the origins of health, promoting the maintenance and strengthening of well-being. The model focuses on problem-solving and the search for solutions, identifying general resources of resilience that enable people to move toward positive health 13.
Empirically, articles were identified whose findings demonstrate the relationship between a high quality of life and a greater tendency to adopt healthy behaviors, also showing that social support improves the perception of health and well-being in adults with CVDs 14.
In the implementation of a salutogenesis model, various key actors are involved, such as the community, which ultimately must be capable of co-producing health and increasing community social capital. Thus, the model encourages communities to focus on mobilizing local strengths or assets, valuing the resources and assets of individuals and communities 15.
For the salutogenic models to have an impact, they must be approached from the perspective of developing public health policies and programs that incorporate this positive health approach to contribute to the promotion of people's health, through the implementation of strategies aimed at correcting eating habits, such as conducting research in this area 12.
In Chile, the evaluation of government programs, together with community and regional evaluations, has enabled the identification of key areas for improvement in the Health Promotion Program, highlighting the need to allocate resources with a focus on equity, optimize spending, improve the efficiency of activities, and strengthen the implementation of the system. In addition, the importance of better coordinating community planning tools, defining regional profiles, and designing quality indicators to evaluate results is emphasized. It is also recommended that studies should be conducted on local health needs and that the program's problem tree should be updated, integrating a gender perspective. These aspects will be addressed during the current three-year period, to ensure access to healthy environments, consider the social challenges that affect health and ensure the right of all to achieve their maximum health potential 16.
Given that social exclusion continues to increase worldwide and is a key factor in perpetuating health inequalities, the implementation of participatory health promotion strategies is a key tool for reversing this tendency. Populations experiencing social exclusion often face barriers to accessing essential services such as healthcare, education, social capital, community connection, housing, and other essential resources. Therefore, it is vital that health leaders and professionals commit to strengthening communities through health actions, creating the necessary conditions to foster community participation and empowerment 17.
Regarding the economic aspects associated with a promotional model, there are few studies in the literature addressing the theme. However, the adoption of preventive health interventions focused on promotion and education to avoid hazardous behaviors can generate significant long-term savings by reducing the need for costly treatments associated with chronic diseases 18. Thus, it is assumed that, while it is true that disease care is important, it entails a series of significant limitations that call into question its ability to respond to the current health scenario of the population and its value over disease prevention and health promotion. Some of these limitations are expressed in high economic and human costs; increasingly complex problems, such as difficulties in acquiring medications and sophisticated equipment; large health inequalities, especially in the most disadvantaged social groups, and the exhaustion of the effectiveness of the direct care model regarding the magnitude and quality of health problems 19.
Given the above, the objective of this study is to identify the gaps, assets, and challenges in the care of hypertension and type II diabetes from the perspective of people who belong to hypertension and diabetes associations and healthcare professionals.
The health assets of a community enable people to recognize the importance and necessity of actively participating in their own health care. In this regard, the asset-based community development (ABCD) approach has been widely used to map local assets and ensure the participation of local communities in public health promotion strategies 20.
As part of a movement to shift public health practices toward addressing health inequalities and inequities, community participation and participatory practices have become more central to health promotion strategies in recent decades.
The relevance of the study lies in advancing the implementation of a salutogenesis model in Chile, with a high impact on people's health, especially those associated with CVDs with high morbidity and mortality rates, through which patients commit to their actions and strengthen their self-care as active members of health to identify and map assets in the community that contribute to improving and/or maintaining people's health. In turn, the research is based on the work of Dorothea Orem, who presents her self-care deficit nursing theory as a general model, composed of three related theories: the self-care theory, which describes why and how people care for themselves; the self-care deficit theory, which describes and explains how nursing can help people; and nursing systems theory, which describes and explains the relationships that must be maintained 21, conceiving the human being as a biological, rational, and thinking organism, with the capacity to reflect on their own experience and on collateral events to perform dependent self-care actions 22. In this context, Orem's theory provides a practical framework for addressing the limitations that people may have in their self-care capacity. While salutogenesis focuses on the resources and factors that promote health, Orem's theory complements that perspective by providing the tools to intervene when these resources or self-care capacities are insufficient. In particular, for dependent self-care in patients with CVDs, Orem's theory explains how nursing intervention can support these individuals in improving their health, within a salutogenesis approach.
Material and Methods
From the early stages of this study, the need for a participatory approach was recognized, a decision that emerged after a process of dialogue between the research team, community healthcare professionals (nurses and local agents), and representatives of patient associations. In this context, it was found that the ABCD model and the participatory action research paradigm adequately addressed the need to highlight the experiences, resources, and challenges from the perspective of those living with chronic noncommunicable diseases (HBP and type II diabetes), while promoting their participation in identifying community resources and solutions.
Regarding the data collection techniques, semi-structured in-depth interviews and focus groups were used, the latter being conducted with participants belonging to the community group of type II diabetics. Both techniques were designed based on a semi-structured questionnaire developed according to the principles of the ABCD model, which focuses on the strengths and resources of the community, collaboration, and collective action. The questions included: How do people interact with professionals when they have a health problem related to hypertension and type II diabetes? What are the institutions and organizations that people usually seek help from? What are the challenges in providing care for these chronic noncommunicable diseases?
The sample was selected through intentional sampling and consisted of twelve users belonging to community associations diagnosed with HBP and/or type II diabetes, and eight healthcare professionals working in community services or providing care for these diseases.
To analyze the information, content analysis was used in the following stages: a) complete the transcription of interviews and focus groups, with content validity review; b) open coding: segmentation of data into units of meaning, assignment of codes; c) grouping into relevant thematic categories, facilitating the understanding of the phenomenon under study; d) analysis of the role of key actors, both formal (health centers) and informal (community leaders), positioning them within the map of community assets; e) comparative analysis between participants' and professionals' responses, identifying similarities and differences in their perceptions and experiences.
The research was conducted in compliance with the ethical principles proposed by Ezequiel Emanuel. It was approved by an accredited ethics committee, and all participants provided informed consent. In turn, the study incorporated participatory ethics, promoting the active involvement of community actors from the formulation of the research question to the validation of results. This practice is aligned with the principles of the ABCD approach, recognizing the community as a co-producer of knowledge, and not just as an object of study 23.
Results
Of the 20 participants, 12 were community members diagnosed with high blood pressure or diabetes mellitus. Within this group, 42 °% were working in education (n = 5), 33 °% in public service offices (n = 4), 8 °% in the health sector (n = 1), 8 °% in social services (n = 1), and another 8 °% in various entities or departments (n = 1). This distribution shows the diverse employment status of the community participants, which favors a broad and contextualized perspective on the challenges of self-care and health promotion in daily environments. The remaining eight professionals were healthcare professionals, including physical therapists, pharmacists, nurses, medical technologists, and physicians. The gaps are described in Table 1.
Table 1 Gaps in Care for Hypertension and Type II Diabetes: Perspectives from Association Participants and Healthcare Professionals
Priority |
Care Needs According to |
Care Needs According to |
Combined Need (Individual Responses) |
Analysis |
|---|---|---|---|---|
1 |
Lack of community-based comprehensive care initiatives. |
Lack of collaborative treatment approaches. |
Lack of teamwork between professionals and patients. |
Need for an integrated approach and joint efforts. |
2 |
Lack of meeting spaces for mutual support. |
Lack of group activities to promote health. |
Need for group environments that promote learning and integration. |
Lack of spaces for sharing experiences. |
3 |
Lack of awareness of the impact of family care on health. |
Lack of complete understanding of the disease, both individually and within the family. |
Limited awareness of family care and the implications of the disease. |
Lack of awareness regarding the disease, which hinders self-care and mutual support. |
4 |
Absence of physical activity programs adapted to chronic diseases. |
Lack of support from family members for treatment follow- up. |
Imbalance between physical needs and adequate family support. |
Lack of organized physical activity programs for patients. |
5 |
Communication gaps regarding community health activities. |
Lack of appreciation for cultural practices related to care. |
Misinformation regarding care opportunities. |
Information disconnection. Need to value cultural care practices. |
6 |
Limited access to transportation to healthcare centers, especially in rural areas. |
Connectivity issues for patients in areas with high geographical dispersion. |
Inequality in access to healthcare services due to geographical and logistical barriers. |
Need to rethink care models, considering infrastructure and logistical resources for access to healthcare centers. |
Source: Prepared by the authors.
Regarding the assets for the care of hypertension and type II diabetes, the variability of the participants' opinions enabled the identification of representative health assets in the community to subsequently create the asset map, in which participants discover the network of relationships and support that together contribute to the maintenance of care for hypertension and type II diabetes 24.
The map allows for the collective construction of knowledge, based on the premise that it is the people themselves who know their territory and its problems best. Mapping helps to strengthen community belonging, as well as the geographical and sociocultural heritage of populations through participatory processes.
Figure 1 Analysis of the Asset Map for the Care of Hypertension and Type II Diabetes
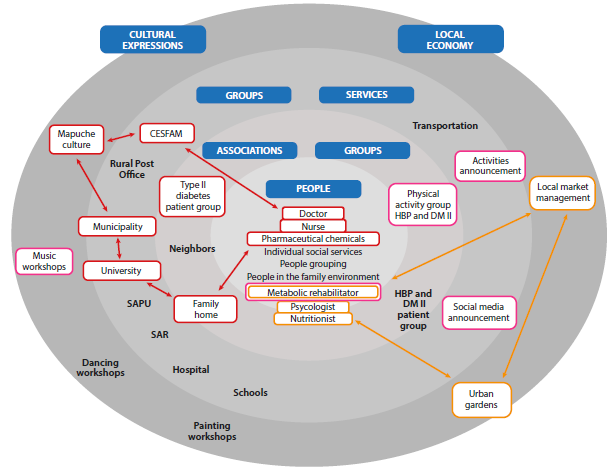
Source: Prepared by the authors
The map reveals the strengths present in the community, but it also highlights the areas where resources are insufficient. For instance, there are gaps in specialized services or educational support, especially in rural or less developed areas. Areas with reduced access to these services and programs face greater challenges in managing chronic diseases such as hypertension and type II diabetes. This situation emphasizes the urgency of designing integrated, localized, and more inclusive care strategies that address inequalities in access to care and strengthen support networks for patients and care providers.
The map highlights the following connection lines, which focus on specific areas to promote better access to and management of healthcare in the community:
- Red: The actors highlighted in red are identified as responsible for promotion and prevention activities, with the connection represented by the red lines between them being crucial. Among the key connections in this process, the work of pharmaceutical chemists with the diabetes group stands out, as does the collaboration with Casa de la Familia, a university-based community project that connects students with the community through health promotion interventions. Although the connection between professionals is recognized, it is suggested that interventions adapted to cultural contexts should be integrated, and there is also a desire for planned promotion activities that respond in a more structured way to the needs of the community.
Create a schedule of activities that is not just a list of tasks, such as "we have this activity and we have to give this talk", but rather one that lets them know that these things are there, so they do not have to keep reminding them. It should be more organized and include various activities with different professionals. (E2)
Then, in addition, our culture of not seeking medical advice in time, whether out of fear, ignorance, or mistrust of Western medicine and placing much more trust in traditional medicine than in the other, leads to appointments being made much, much too late, and interventions must be planned accordingly. (E10)
We have a pharmaceutical chemist who helps us. He helps us, he is registered as an equal partner, he gives us talks every month, he is part of the group, he cares about us. (E12)
- Yellow: The actors highlighted in yellow represent those who are in the territory. However, some are not identified by the community, which also demonstrates the weak connection between them. The relationship between the yellow lines arises from the narratives regarding the possibility of interventions that enable the implementation of sustainable and adequate nutrition, with cultural relevance for patients with hypertension and type II diabetes. The challenge remains to implement local markets and urban gardens, with the participation of volunteer farmers and community residents.
If one were to add two more psychologists, one could solve the problem, along with materials. A slightly larger space is needed, and it is always necessary to hire more professionals, but sometimes the budget is not available. (E2)
- Purple: The actors highlighted in purple correspond to assets related to the promotion of physical activity. The purple lines focus on the connection between health assets for promoting physical activity. The metabolic rehabilitation specialist states that there is still insufficient space to accommodate a larger number of users, although systematic work has been conducted with users who are admitted each year. It should be noted that the diabetic group is unaware of the metabolic rehabilitation asset and also finds it difficult to connect with activities.
Regarding the results of the challenges, the following metacatego-ries and subcategories were identified (Table 2).
Table 2 Active Challenges for the Care of Hypertension and Type II Diabetes
Metacategory |
Subcategories |
|
|---|---|---|
Challenges |
From a reactive to a proactive approach to health management. |
Healthcare actions based on welfare. |
Removing barriers to access and logistics. |
Language and access barriers dominated by social determinants. |
|
Search for connections between community resources. |
Inconsistency, physical activity removed from programs. |
Source: Prepared by the authors.
Challenges - Metacategory: From a Reactive to a Proactive Approach to Health Management; Subcategory: Welfare-Based Health Actions
We are conducting group checkups, and we are trying to educate people, but I think we need to reach out more to the community, rather than having the community come to us. We need to go to schools and neighborhood associations and provide more education, with a particular emphasis on younger people. (E2)
I believe it has more to do with that, with education. I believe that primary care has to do with that. Right now, we are very welfare-oriented. The patient comes in, the doctor prescribes medication, but we are failing in the other part, which is primary care. We criticize ourselves. This is what is failing: making the patient aware of the disease. (E5)
Both excerpts reveal a core criticism of the traditional health education strategy, which relies on people seeking health services rather than services reaching people. Here, a more active, community-based approach is proposed. The mention of going to schools and neighborhood associations shows a focus on preventive education and health promotion outside of healthcare centers, in places where the community is naturally present. The excerpt proposes a paradigm shift in seeking the community to educate it and reflects the current need for transformation of the health system, insisting on a proactive approach that involves the community with a preventive focus on "younger people," thus signaling the importance of early education.
The criticism also highlights that the current primary care model is unbalanced, as it focuses mainly on treating the symptoms of diseases, while neglecting health education and raising patient awareness of their own illness. This could be contributing to inadequate management of long-term diseases and a lack of patient empowerment.
On the other hand, self-criticism among healthcare professionals has been enriched, as they recognize the need to deepen their working methodologies to improve health management.
Challenges - Meta-Category: Removing Barriers to Access and Logistics; Subcategory: Language and Access Barriers Dominated by Social Determinants
Although a high percentage of the rural population is registered in the CESFAM, there are logistical challenges, such as limited transportation schedules, that impede many patients from attending their check-ups. If they are unable to attend in the morning, it is difficult for them to reach the CESFAM due to the lack of transportation options during the rest of the day. (E3)
In rural areas, language barriers, such as the fact that some patients only speak Mapudungun, make it difficult to communicate the importance of checkups and tests, despite the presence of an intercultural facilitator. Although patients in urban areas are more accessible, lack of knowledge regarding the disease remains a challenge. The difficulty lies in the fact that, even when explained to them, they do not always fully understand, which limits their ability to perform self-care and hinders the effectiveness of professional care. (E2)
We never have enough time to see all our patients. Most of our population is rural, with only 10 % living in urban areas and 90 % in rural areas, which means that many come from very far away. When they arrive, there are often no appointments available, which is frustrating for them. In addition, they face additional difficulties such as poverty and lack of public transportation, as they often do not have access to buses or other means of transportation to get to the health center. (E5)
The interventions reveal critical challenges in the search for more equitable primary care, where rural contexts are not affected, and therefore highlight what hinders access for communities, such as the lack of transportation options and limited medical care hours. Additionally, there are cultural barriers, such as language, which hinder effective communication. Despite having an intercultural facilitator, there are barriers such as a lack of understanding of the disease and the importance of check-ups, which affect patients' ability to adopt self-care practices. The social determinant of poverty also presents a significant barrier, as it limits access, thereby perpetuating health inequality. These factors combined create a cycle of social and health exclusion that impacts the health of rural communities, requiring a comprehensive approach that addresses logistical, cultural, and socioeconomic barriers to improve access to healthcare.
Challenges - Metacategory: Search for Connections between Community Resources; Subcategory: Inconsistency, Physical Activity Removed from Programs
There are no sports activities specifically aimed at them at the community level. However, we do have an adapted sports program in collaboration with the university's sports technician program, in which some of the patients actively participate. Despite this effort, participation is not universal, as not everyone has access to this program. It is worth noting that this initiative comes from the university and is not part of a formal policy implemented at the community level. (E4)
We do not have direct contact with the diabetes association, despite the fact that the program has been in place for several years. Indeed, sometimes even the associations themselves are not fully informed about the benefits available. I understand that some people are aware of these services, but I have not had the opportunity to introduce myself directly, as the necessary steps have not been taken to facilitate this contact. (E6)
Previously, there was an item in the RAYEN system, REM 27, which corresponded to the group physical activity workshop of the cardiovascular program. However, this item was removed this year. (E8)
It would be important to provide more recreational activities. People are also aware of the workshops held at the sports center, and patients could be informed about these options. Despite this, the activities available are not specifically designed or tailored to meet the specific needs of chronic patients, which limits their focus and effectiveness. (E1)
Connection and accessibility to community resources in the context of primary health care are challenges highlighted by participants. Although there are initiatives to establish links with universities related to physical exercise, access is not universal. In addition, it was mentioned that the lack of adequate measures to facilitate interaction between healthcare professionals and associations represents a significant barrier. Professionals also mention the elimination of the group physical activity workshop in the RAYEN system (information system), which reflects a lack of continuity and consistency in the available resources. Such changes can lead to confusion and misinformation among users, who may not be aware of the elimination of the service. Finally, although there are other recreational options in the various sports centers, the activities are not specifically designed to meet the needs of chronic patients, which limits their effectiveness. This fact highlights the importance of creating and offering more focused and differentiated activities, adapted to the conditions of patients, to improve their participation and results in health programs.
Discussion
This study highlights several limitations: Lack of collaboration between professionals and patients; need for group settings that promote learning and integration; limited awareness of family care and the implications of the disease; imbalance between physical needs and adequate family support; misinformation regarding care opportunities; inequality in access to health services due to geographical and logistical barriers.
Concurrently, there are gaps in specialized services and educational support, especially in rural areas. This situation highlights the urgency of designing integrated, localized, and more inclusive care strategies that address inequalities in access to care and strengthen support networks for patients and care providers.
Similarly, one study found evidence that demographic factors, social risk factors, and adverse health behaviors were associated with chronic diseases and mental health problems. Associated social factors included low educational level, rural residence, income inequality and unemployment, poverty, limited social capital, stressful life events, and low use of health services 25. On the other hand, globally, the main determinant of access to primary care services for older people living in rural areas is the lack of availability of services. However, it is worth noting that barriers to access in rural areas of different countries vary in degree, depending on the level of social organization that prevails 26.
In this regard, a study on interventions aimed at optimizing the management of hypertension and type II diabetes highlights the importance of comprehensive approaches that combine patient education, medication management, and lifestyle changes. In addition, technology-based interventions (mobile applications and telemedicine) are effective in improving treatment adherence. The study also emphasizes the need for greater training for professionals and clear protocols to ensure more effective and sustainable management of these chronic conditions 27.
An additional study indicates that loneliness and social isolation are associated with increased morbidity, including cardiovascular problems, cognitive impairment, and increased mortality, with contributing factors including the loss of loved ones, mobility issues, and changes in social networks. The importance of promoting social connections and community support is emphasized, recommending socialization programs and the use of technology to maintain contact and inclusion among adults 28.
On the other hand, the asset map, as an operational tool, describes the assets and connection lines that focus on promoting better access to and management of health in the community.
Among the actors responsible for promotion and prevention activities (red), the professional role of the pharmaceutical chemist stands out, whose work involves collaboration with the diabetes group, as well as collaboration with the Casa de la Familia, recognizing the connection between professionals. However, it is suggested that interventions should be adapted to cultural contexts, and there is also a desire for planned promotion activities that respond in a more structured way to the needs of the community.
The actors in yellow are present in the territory, although some are not identified by the community, evidencing a weak connection between them, which suggests interventions that allow for the implementation of sustainable and adequate nutrition, with cultural relevance in patients with hypertension and type II diabetes. The implementation of local markets and urban gardens, with the participation of volunteer farmers and community residents, remains a challenge.
Finally, the actors in purple correspond to assets related to the promotion of physical activity. Regarding this, the metabolic rehabilitation specialist reports that there is not enough space to welcome a larger number of users. It should be noted that the diabetic group is unaware of the metabolic rehabilitation asset and also has difficulty connecting these activities.
On this topic, an asset-based study looks at the experiences and perspectives of men living with HIV, considering not only their vulnerabilities but also the resources and abilities they have to deal with this situation. In the findings, men reported having developed a number of personal and social assets that enabled them to rebuild their lives in a positive way, including social support from family and friends, access to health services, and the adoption of new ways of managing HIV emotionally and psychologically. In addition, some men were actively engaged in raising HIV awareness and worked to challenge the stigma associated with the disease. It is suggested that an asset-based approach may be more effective in supporting people living with HIV, as it helps to empower them rather than focusing solely on their deficiencies 29.
An article examines the relationship between physical activity, sedentary behavior, and health-related quality of life in adults, revealing that higher levels of physical activity are associated with a better quality of life, while prolonged time spent in sedentary activities is related to a decrease in general well-being. The findings suggest that promoting physical activity and reducing sedentary behavior are essential for improving quality of life in the adult population 30.
Another study indicates that older people who participate in regular physical activity report lower levels of depression and anxiety, as well as a more positive perception of their quality of life. The study suggests that community interventions that encourage exercise could have a significant impact on people's quality of life. In addition, it emphasizes the need to consider individual and community factors when designing physical activity programs for older people 31.
Regarding the participation of vulnerable populations with an asset-based approach, this provides a positive perspective on the capacities and resources that can be developed. The findings indicate that participation in community groups has a positive impact on vulnerable people in terms of empowerment, as participants experience an increase in their sense of control over their lives and their ability to influence their environment; social networks, since participation contributed to strengthening networks and increasing available social support; greater emotional well-being, as people reported greater emotional satisfaction and self-esteem, stemming from a sense of belonging and community support; and skills development, since community groups offer opportunities to learn new skills, which contributes to autonomy and personal growth.
Asset-based approaches are effective in improving the quality of life of socially vulnerable populations. The key is to recognize and build upon the resources that these individuals already possess, rather than focusing solely on their deficiencies or problems. By encouraging participation in community groups, a sense of belonging is promoted and social cohesion is strengthened, which is essential for reducing exclusion and improving the integration of these groups into society. The authors suggest that public policies and social programs should adopt asset-based approaches to promote more effective inclusion of vulnerable populations, helping them to leverage their personal and social strengths rather than focusing solely on their needs or limitations 32.
In addition, an asset-based approach can be used for sustainable local economic development in various communities, including rural areas, small towns, and urban areas. Active community participation is key to improving quality of life and creating economic development that does not rely exclusively on external resources but rather uses the community's internal strengths. The findings suggest that communities that implement an asset-based approach improve their quality of life, fostering community empowerment, sustainable economic development, and greater social cohesion 33.
Finally, at the community level and among healthcare professionals themselves, there is a shared understanding of the need to address issues that limit care and lead to a deterioration in the health of the chronically ill population. In this sense, it is worth noting that identifying gaps is key to conceiving improvement options that are seen as opportunities for developing comprehensive healthcare with a focus on the family healthcare model currently in place in primary care, and with active patient participation.
Currently, the main challenges lie in accessing care and the availability of primarily promotional and preventive services. Therefore, the challenge is to bring care closer to patients, eliminating the need for them to travel constantly.
In this context, an option that has become increasingly popular is telemedicine. This is evidenced by various studies in which patients report feeling more comfortable with these arrangements, with their emotional and physical needs being met. In addition, they emphasize that telemedicine allows them to avoid unnecessary travel, save time, and stay at home, where, in many cases, their families have supported them in using technology when they have needed it 34. Other programs, such as the primary care resolution program, aim to improve the quality and quantity of services provided so that it is possible to advance comprehensive patient care in areas such as ophthalmology, otolaryngology, and diagnostic support, among others 35.
Unfortunately, it is well known that healthcare resources are limited and that there are often complexities involved in hiring more personnel, which is why making optimal use of consultation hours is essential to better manage demand. For this purpose, the current challenge is to seek effective demand management measures through local teams, making controlled use of available resources and optimizing consultation hours and resolution channels. In Chile, the telehealth platform allows for remote demand management, preventing patients from waiting in line and providing unrestricted access to request care, which will be reviewed by a professional who will determine a resolution pathway and priority for the request 36.
Primary health care has a key role in leading education, health promotion, and disease/injury prevention efforts in the community. These practices are vital for providing care to people with chronic noncommunicable diseases, since health promotion focuses not only on the disease but also on the living conditions of individuals and their families. In this sense, and recognizing the importance of patient participation in the care and protection of their health, the research is based on Orem's self-care theory, which emphasizes that self-care is essential for identifying the potential capabilities of individuals, allowing them to meet their needs to maintain life and health, recover from damage and illness, and manage the effects of these 37.
It is therefore necessary to control HBP and type II diabetes mellitus through prevention, early diagnosis, and timely and adequate treatment to avoid complications. This is where self-care, through structured educational interventions based on the identification of individual needs, expectations, knowledge, and beliefs, combined with the empowerment of the individual, will enable the achievement of permanent behaviors that facilitate self-knowledge, behavior modification, and the acquisition or relearning of knowledge and skills 38.
Conclusion
The study addresses objectives related to gaps, asset development, and challenges. The results contribute to an analysis of public policies related to the issue and the establishment of new health models, with a promotional approach, to reduce the burden of disease in hypertension and type II diabetes and its impact on physical, social, and mental health, as well as individual, family, and social health, as a way to contribute to a healthier and more proactive environment.
Furthermore, the need for public health policies that promote active lifestyles is reinforced, as is the importance of interventions that integrate increased physical activity and reduced sedentary time.
Asset-based local development and community participation are powerful strategies for improving quality of life, particularly for people with chronic diseases such as hypertension and type II diabetes, in a range of contexts.
Through the identification and use of each community's internal resources, whether human, cultural, natural, or economic, it is possible to create more inclusive, equitable, and sustainable development.
It is recommended that organizations and planners adopt asset-based approaches to support local economic development, allowing communities to control their own destiny and foster innovative solutions tailored to their specific needs, and it is recommended that these approaches be integrated into public policies to maximize impact at the local level.
Conflict of interest: The authors declare that they have no conflicts of interest.
References
1. Organización Panamericana de la Salud. La carga de enfermedades cardiovasculares - OPS/OMS [Internet]; 2023. https://www.paho.org/es/enlace/carga-enfermedades-cardiovasculares
2. Varleta P, Acevedo M, Valentino G, Brienza S, Mildren del Sueldo. Conciencia de enfermedad cardiovascular y conocimiento sobre factores de riesgo y prevención cardiovascular: resultados chilenos de encuesta SIAC Cono Sur. Rev Chil Cardiol [Internet]. 2022;41(2):82-91. DOI: https://doi.org/10.4067/S0718-85602022000200082
3. Organización Mundial de la Salud (OMS). Primer informe de la OMS detalla el impacto devastador de la hipertensión y las formas de detenerla. Organización Mundial de la Salud; 2023. https://www.who.int/es/news/item/19-09-2023-first-who-report-details-devastating-impact-of-hypertension-and-ways-to-stop-it?utm_source=
4. Organización Panamericana de la Salud. Hipertensión - OPS/OMS [Internet]; 2023. https://www.paho.org/es/temas/hipertension
5. World Health Organization (WHO). Hypertension [Internet]. Geneva: World Health Organization; 2021. https://www.who.int/es/news-room/fact-sheets/detail/hypertension
6. Snarska K, Chorąży M, Szczepański M, Wojewódzka-Żeleznia-kowicz M, Ładny JR. Quality of life of patients with arterial hypertension. Medicina [Internet]. 2020;56(9):459. DOI: https://doi.org/10.3390/medicina56090459
7. Organización Mundial de la Salud. Diabetes [Internet]; 2023. https://www.who.int/es/news-room/fact-sheets/detail/diabetes
8. Organización Panamericana de la Salud. Diabetes - OPS/OMS [Internet]; 2021. https://www.paho.org/es/temas/diabetes
9. Organización Panamericana de la Salud. Ante aumento número casos en todo el mundo que se han cuadruplicado en los últimos decenios; 2024. https://www.paho.org/es/noticias/14-11-2024-ante-aumento-numero-casos-todo-mundo-que-se-han-cuadruplicado-ultimos-decenios
10. Kempf K, Hennings L, Wendt L, et al. Psychological and quality of life aspects of patients with type 2 diabetes: A longitudinal study. Diabetes Therapy. 2020;11(6):1199-1211. DOI: https://doi.org/10.1007/s13300-020-00832-x
11. Balcázar G, Liendo J, Fernández M. Salutogenesis and cardiovas-cular health in adults: A scoping review [Internet]; 2020. https://www.researchgate.net/publication/338730670_SALUTOGENE-SIS_AND_CARDIOVASCULAR_HEALTH_IN_ADULTS_A_SCOP-ING_REVIEW
12. Alarcón Alfonso CM. La salutogénesis y su aplicación en la educación. Educación y Desarrollo. 2020;20(1):1-10. Disponible en: https://ciberindex.com/index.php/ed/article/view/11509ed
13. García M, Pérez L, Rodríguez J. Sentido de coherencia en las en-fermedades crónicas: una revisión integradora. ResearchGate; 2023. https://www.researchgate.net/publication/374245242_Sentido_de_coherencia_en_las_enfermedades_cronicas_una_revision_integradora
14. Parra DI, Romero LAL, Cala LMV. Calidad de vida relacionada con la salud en personas con hipertensión y diabetes mellitus. Enferm Global [Internet]. 2021;20(2):316-44. DOI: https://doi.org/10.6018/eglobal.423431
15. Faúndez-Pino LF. Envejecimiento saludable y enfoque saluto-génico. Rev Mex Med Fam [Internet]. 2023;10(1). DOI: https://doi.org/10.24875/RMF.22000090
16. Ministerio de Salud de Chile. Orientaciones técnicas de planes trienales de promoción de la salud 2022-2024 [Internet]. Santiago: Ministerio de Salud; 2024. https://entornospromo-toresdelasalud.minsal.gob.cl/wp-content/uploads/2024/05/ORIENTACIONES-TECNICAS-DE-PLANES-TRIENALES-DE-PROMOCION-DE-LA-SALUD-2022-2024.pdf
17. Siersbaek R, O’Donnell C, Parker S, Ford J, Burke S, Cheallaigh CN. Social exclusion and its impact on health over the life course: A realist review protocol. HRB Open Res [Internet]. 2023;6:34. DOI: https://doi.org/10.12688/hrbopenres.13746.2
18. Micha, R., Peñalvo, J. L., Cudhea, F., Imamura, F., Rehm, C. D., & Mozaffarian, D. (2017). Association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes in the United States. JAMA, 317(9), 912-924. DOI: https://doi.org/10.1001/jama.2017.0947
19. Solano Siles A. La promoción de la salud [Internet]; s.f. https://www.binasss.sa.cr/revistas/ts/63/art2.htm
20. Agdal R, Midtgård IH, Meidell V. Can Asset-Based Community Development with Children and Youth Enhance the Level of Participation in Health Promotion Projects? A Qualitative Meta-Synthesis. Int J Environ Res Public Health. 2019;16(19):3778. DOI: https://doi.org/10.3390/ijerph16193778
21. Naranjo-Hernández Y. Modelos metaparadigmáticos de Dorothea Elizabeth Orem. Rev Arch Med Camagüey [Internet]. 2019;23(6):814-25. https://www.redalyc.org/journal/2111/211166534013/html/
22. Cano MC, Escartín TM, Campillo MM, Francés VMA. Iniciación en el mapeo de activos en un centro de salud urbano de Zaragoza. Deleted J [Internet]. 2023;80. DOI: https://doi.org/10.55783/comunidad.250305
23. Whiting L, Kendall S, Wills W. An asset-based approach: An alternative health promotion strategy? [Internet]. Research Gate. https://www.researchgate.net/publication/233725923_An_asset-based_approach_An_alternative_health_promotion_strategy
24. Pola-García M, Domínguez-García M, Gasch-Gallén Á, Lou-Alcaine ML, Enríquez-Martín N, Benedé-Azagra CB. Implementación de un protocolo de recomendación formal de activos para la salud en los equipos de atención primaria aragoneses. Aten Prim. 2023;55(4):102535. DOI: https://doi.org/10.1016/j.aprim.2022.102496
25. Devassy SM, Benny AM, Scaria L, Nannatt A, Fendt-Newlin M, Joubert J, et al. Social factors associated with chronic non-communicable disease and comorbidity with mental health problems in India: a scoping review. BMJ Open [Internet]. 2020;10(6):e035590. DOI: https://doi.org/10.1136/bmjopen-2019-035590
26. Santoyo Sánchez G, Arredondo-López AA. Revisión y análisis sobre los determinantes de acceso a los servicios de atención primaria en población adulta mayor rural y urbana. Horiz Sanit. 2020 May 27;19(2):175-84. Disponible en: https://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S2007-74592020000200175
27. González de León B, León Salas B, Del Pino-Sedeño T, Rodríguez-Álvarez C, Bejarano-Quisoboni D, Trujillo-Martín MM. Aplicaciones móviles para mejorar la adherencia a la medicación: revisión y análisis de calidad. Aten Primaria [Internet]. 2021;53(9):102095. DOI: https://doi.org/10.1016/j.aprim.2021.102095
28. National Institute on Aging. Soledad y aislamiento social: Consejos para mantenerse conectado [Internet]; s. f. https://www.nia.nih.gov/espanol/soledad-aislamiento-social/soledad-aislamiento-social-consejos-mantenerse-conectado
29. Fauk NK, Mwanri L, Gesesew HA, Ward P. Biographical reinvention: an asset-based approach to understanding the world of men living with HIV in Indonesia. Int J Environ Res Public Health. 2023;20(16):6616-6. DOI: https://doi.org/10.3390/ijerph20166616
30. Goberdhan S, Gobin R, Perreira O, Sharma M, Ramdeen M, Harding S. Formative exploration of the feasibility of embedding community assets into primary health care: barbershop and place of worship readiness in Guyana. J Prim Care Community Health [Internet]. 2022;13:21501319221135949. DOI: https://doi.org/10.1177/21501319221135949
31. Seah B, Espnes GA, Ang ENK, Lim JY, Kowitlawakul Y, Wang W. Supporting the mobilization of health assets among older community dwellers residing in senior-only households in Singapore: a qualitative study. BMC Geriatr. 2020;20(1). DOI: https://doi.org/10.1186/s12877-020-01810-6
32. Corrigan O, Hughes S, Danielsen S, Doherty S, Kabir R. The impact of engaging with community groups: Asset-based approaches and the lived experience of socially vulnerable populations in the UK. Front Public Health [Internet]. 2023;11. DOI: https://doi.org/10.3389/fpubh.2023.1156422
33. Kammer-Kerwick M, Takasaki K, Kellison JB, Sternberg J. Asset-based, sustainable local economic development: Using community participation to improve quality of life across rural, small-town, and urban communities. Appl Res Qual Life. 2022. DOI: https://doi.org/10.21203/rs.3.rs-1138803/v1
34. Huaiquián Silva, J., Espinoza Venegas, M., & Ríos Bolaños, M. (2022). Salud digital en el control de pacientes crónicos durante la pandemia: La mirada del equipo de salud. Ciencia y Enfermería, 28, 32. http://dx.doi.org/10.29393/CE28-32SDJM30032
35. Programas de Resolutividad | Dirección de Salud [Internet]; 2025 https://www.saludstgo.cl/servicios/programas-de-resolutividad/
36. Ministerio de Salud Chile. Telesalud: Así funciona la estrategia de gestión remota de la demanda en la red del Servicio de Salud Metropolitano Central. MINSAL; 2024. https://portalsalud-digital.minsal.cl/telesalud-asi-funciona-la-estrategia-de-gestion-remota-de-la-demanda-en-la-red-del-servicio-de-salud-metropolitano-central/
37. De Carvalho EA, Júnior TTDN, Nogueira ILA, De Assis Silva CJ, De Queiroz AAR, De Menezes RMP. Autocuidado de usuarios con enfermedades crónicas en la atención primaria a la luz de la teoría de Orem. Enferm Global [Internet]. 2022;21(4):172-215. DOI: https://doi.org/10.6018/eglobal.508511
38. Herrera Molina AS, Mendoza G, Herrera Molina AS, Mendoza G. Estrategia educativa intercultural de enfermería en el autocuidado del adulto hipertenso. Rev Cub Reumatol [Internet]. 2022;24(2). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1817-59962022000200018