Individual and Group Education in Diabetes and Outcomes
Educación individual y grupal sobre la diabetes y sus resultados
Educação individual e grupal sobre a diabete e os resultados
Recibido: 17 de julio de 2013
Enviado a pares: 26 de agosto de 2013
Aceptado por pares: 10 de enero de 2014
Aprobado: 10 de abril de 2014
DOI : 10.5294/aqui.2014.14.2.1
Elif Ünsal-Avdal1
Burcu Arkan2
1 PHD. Asistant Professor, Izmir Katip Çelebi University, Turkey.
2 Lecturer. Uludag University, Turkey.
To reference this article / Para citar este artículo / Para citar este artigo
Ünsal-Avdal E, Arkan B. Individual and Group Education in Diabetes and Outcomes. Aquichan 2014; 14(2):138-147, DOI : 10.5294/aqui.2014.14.2.1
|
ABSTRACT Aim: The purpose of the present study in this context was to review the effect two different types of diabetes education being implemented in an actual setting had on the outcome of care (levels of knowledge, self-care agency, A1c, BMI). Methods: Research was carried out as a correlational and descriptive study. The sample was comprised of 391 persons. The data were collected through diabetic assesment forms, diabetes knowledge assessment forms, the Self-care Agency Scale and A1c and BMI assessment forms. Results: The results indicated the type of educational technique was able to affect levels of knowledge by 77%, self-care agency by 76%, A1c levels by 78% and the BMI by 75%. Conclusions: The delivery of individual and group diabetes education, together, is perceived to be a better method of ensuring an individual's effective self-management. KEYWORDS Education, diabetes mellitus, body mass index, self care, nursing (source: DeCS, BIREME). |
RESUMEN Objetivo: el propósito del presente estudio fue examinar los efectos de las dos técnicas de educación diabética que se estaban implementando en un entorno real sobre los resultados de la atención (los niveles de conocimiento, el manejo del auto - cuidado, A1c , BMI). Métodos: la investigación se llevó a cabo como un estudio correlacional y descriptivo. El muestreo fue compuesto por 391 personas. Los datos se seleccionaron mediante formularios de evaluación diabética, formularios de evaluación de los conocimientos diabéticos, la Escala de Agencia de Autocuidado y formularios de evaluación de Alc y BMI. Resultados: los resultados indicaron que la modalidad de la técnica educativa fue capaz de afectar a los niveles de conocimiento en un 77%, a la agencia de autocuidado en un 76% , a los niveles de A1lc en un 78% y al índice de masa corporal en un 75%. Conclusion: se ve que una combinación de educación diabética individual y grupal es un mejor método para asegurar la autogestión eficaz de un individuo. PALABRAS CLAVE Educación individual, educación grupal, diabetes mellitus, índice de masa corporal, autocuidado, enfermería (fuente: DeCS, BIREME). |
RESUMO Objetivo: o propósito do presente estudo foi examinar os efeitos das duas técnicas de educação diabética que estavam sendo implementadas em um ambiente real sobre os resultados do atendimento (os níveis de conhecimento, o manejo do autocuidado, A1c, BMI). Métodos: a pesquisa foi realizada como um estudo correlacional e descritivo. A amostra foi composta por 391 pessoas. Os dados foram selecionados mediante formulários de avaliação diabética, formulários de avaliação dos conhecimentos diabéticos, a Escala de Agência de Autocuidado e formulários de avaliação de A1c e BMI. Resultados: os resultados indicaram que a modalidade da técnica educativa foi capaz de afetar os níveis de conhecimento em 77%, a agência de autocuidado em 76%, os níveis de A1c em 78% e o índice de massa corporal em 75%. Conclusão: vê-se que uma combinação de educação diabética individual e grupal é o melhor método para garantir a autogestão eficaz de um indivíduo. PALAVRAS-CHAVE Educaçao, diabetes mellitus, índice de massa corporal, autocuidado, enfermagem (fonte: DeCS, BIREME). |
Introduction
Diabetes is a disease that is becoming increasingly more prevalent (International Diabetes Federation, 2012; International Diabetes Federation, 2011). In 2002, there were approximately 171.2 million diabetics around the world and this figure is expected to double by 2030 (Wild, Roglic, Gren & et al., 2004; International Diabetes Federation, 2011). Because of its acute and chronic complications, diabetes is a high-cost disease, but the emergence of complications can be reduced through effective metabolic control (International Diabetes Federation, 2012; American Diabates Association, 2012).
Self-care refers to actions and attitudes that contribute to the maintenance of well-being and personal health and promote human development (American Diabates Association, 2012). Diabetes self-care is essential to effective metabolic control. Self-care agency is a human aptitude that involves "the ability for engaging in self-care. Self-management has become a popular term for behavioral interventions, as well as for healthful behavior (American Diabates Association,2012). Self-management education is necessary to ensure diabetes self-care (American Diabates Association, 2012; Funnell,Brown, Childs & et.al., 2007). Diabetes self-management serves to enable the patient to make educated decisions and otherwise supports effective self-care behavior and problem-solving. It also encourages active cooperation with the health team to improve clinical results, general health and quality of life (Bilir & Çagdas, 2004). How education is delivered is important to ensuring its effectiveness. In an article, Bilir refers to one of the leaders in adult education, Eduard Christian Lindeman, who claims educational technique rather than content is of more importance (Medicare Program, 2012). Diabetes self-management education is delivered as a program for individual education or as group education. Both techniques are patient-focused. In individual education, there is one-on-one contact with the individual who has diabetes, and interaction with the specialist is intense.
In group education, individuals with diabetes mellitus share their experiences and problems with one another and a problemsolving approach is implemented more effectively (Bilir & Çagdas, 2004; Funnell,Brown, Childs & et.al., 2007; American Diabates Association, 2012). The group technique delivers education simultaneously to greater numbers of individuals with diabetes mellitus. According to the criteria established by the International Health Care Finance Group, the number of participants in group education is defined as no less than two (2) and 20 at the most. It also saysone group education session is the equivalent of ten individual education sessions (Rickheim, Weaver, Flader & et al., 2002). For this reason, group education is more cost-effective (Norris, Engelgau, Narayan, 2001; Zrebiec, 2003).
Many studies have been conducted on diabetes education techniques. However, their results differ and the most effective education methodology has yet to be defined. Most of the research in this field consists of experimental, randomized controlled studies. The results of a study that defines an actual implementation setting may be useful to the evaluation of other results.
Background
This is especially true for the management of chronic conditions. Diabetes self-management education is delivered as a program for individual education or as group education. Today, the tendency toward group education has increased due to its costeffectiveness. According to the literature, results attained subsequent to individual and group education have been measured and compared and meta-analysis and reviews have been conducted in this context (Norris, Lau, Smith & et al., 2002; Mensing & Norris, 2003; Mannucci, Pala & Rotella, 2005; Deakin, McShane, Cade & et al., 2005; Uttech, 2006; Kulzer Hermanns, Reinecker & et al., 2007; Jarvinen, Juurinen, Alvarsson & et al., 2007; Funnell, Brown, Childs et.al., 2007; International Diabetes Federation, 2011). In 2001, Norris et al. performed a systematic review of randomized control trials and compared the results of individual and group education (Norris, Lau & Smith, 2002). Their studies revealed the teaching of lifestyles and skills was effective in both individual and group education. They also showed the methodology used in some group work was weak, and the recommendation was that more research should be conducted in this area. Norris et al. worked on the same subject again in 2002, conducting a meta-analysis of studies on the effectiveness of diabetes education that were published during 1980-1999 (Mensing & Norris, 2003). The results of their meta-analysis showed there was no significant difference between the effects of group and individual education on glycemic control. In 2003, Mensing and Norris reviewed the work that had been done in 1985-1996 on the effectiveness and implementation of group education (Deakin, McShane, Cade & et al., 2005).
The results of Mensing and Norris's (2003) review indicated quality literature on the effectiveness of individual versus group education was inadequate. They stated the characteristics of both the patient and the educator could affect results, the best format for education had yet to be defined, and both methods had advantages and disadvantages. Again, the recommendation was that more quality studies should be carried out in this area. Deakin et al. (2005), in their 2005 meta-analysis , found group education was effective in improving knowledge levels, fasting blood glucose levels, A1c, blood pressure and drug dependency in patients with type 2 diabetes mellitus (Mannucci, Pala & Rotella, 2005).
Other studies also have displayed differing results. The research results reported by Mannuchi et al. showed a statistically significant improvement in Alc levels and quality of life in individuals with type 1 diabetes who had received interactive group education, compared to patients who had experienced no group interaction (Kulzer, Hermanns, Reinecker & et al., 2007). Kulzer also found group education to be more effective than individual education (Uttech, 2006). On the other hand, Uttech found, in his thesis, that group education had no effect on self-sufficiency, while Jarvinen et al. reported similar effects on glycemic control and treatment satisfaction through individual and group education in patients with type 2 diabetes mellitus who were just starting an insulin regime (Jarvinen, Juurinen, Alvarsson & et al., 2007; International Diabetes Federation, 2011).
The purpose of the present study, in this context, was to review the effects two different types of diabetes education being implemented in an actual setting had on the results of care (levels of knowledge, self-care agency, A1c, BMI).
Material and Methods
Design
This descriptive study was conducted at the endocrinology polyclinics of two university hospitals in Izmir, Turkey.
Participants and Setting
This study was conducted at the endocrinology polyclinics of two university hospitals in Izmir, Turkey. Both polyclinics work from 8:00 a.m. to 5:00 p.m., four days a week, and individuals with diabetes are invited for a checkup and diabetes education every three months. The polyclinics are furnished with diabetes education centers managed by diabetes nurses. Newly diagnosed patients with diabetes mellitus are referred to diabetes nurses. The nurses carry out individual education sessions in accordance with adult education principles and ADA (2012) criteria, so as to ensure the self-management of individuals with diabetes. In addition, group education sessions are planned and implemented every Wednesday. Individual education is repeated two to three times, depending on the patient's needs , and the patient is encouraged to participate in the group sessions on Wednesdays. Group education takes place with about 15-20 patients, although this number is sometimes higher. In the group sessions, specialists (nurses, doctors, dieticians) impart diabetes education answer patients' questions, share experiences and formulate plans for the next group session. However, in spite of this guidance, some patients attend group or individual sessions only sporadically. No more than approximately one third of the patients regularly attend both individual and group education sessions.
The sample for the research included 391 persons between the ages of 19 and 65 who went to the polyclinics (department of a hospital at which outpatients are treated) for routine checkups during the period from January to June 2010, who had been diagnosed with diabetes at least six months before, who consented to volunteering for the study and who had received diabetes education previously. Since patients usually come to the polyclinics for a checkup every three months, the data collection period for both hospitals was defined as three months for each hospital.
Data Collection
This study featured one-time data collection and post-assessment. The data were collected by the researchers during a face-to-face interview in the waiting room, before the patient was called in to see the doctor. The A1c value is average blood glucose control for the past three (3) months; the BMI value is current. The diabetic's A1c and BMI values were obtained from the medical files.
Measures
The data for the research were collected using diabetic assesment forms, diabetes knowledge assessment forms, the Self-care Agency Scale and A1c and BMI assessment forms. The diabetes knowledge assessment form was created by the researchers on the basis of the relevant literature (American Association of Clinical Endocrinologists Guideline, 2012; International Diabetes Federation, 2012). The form was prepared separately for individuals with type 1 and type 2 diabetes mellitus, and contained questions to assess knowledge about diabetes in general, nutrition, exercise, treatment and monitoring. The high total points recorded in the diabetes knowledge assessment form showed the individual with diabetes mellitus has adequate knowledge concerning the disease. The Cronbach alpha coefficient defining reliability of the responses to the questions and homogeneity within the items was found to be 0.88.
The Self-care Agency Scale developed by Kearney and Fleisher is made up of 43 items (Kearney & Fleisher, 1979). It was adapted to the Turkish population by Nahcivan in 1993 (Nahcivan,1993); the items were reduced to 35, with the Kuder-Richardson 20 reliability coefficient calculated as 0.92 (Nahcivan,1993). Pinar, too, worked on the validity and reliability of the scale for chronic diseases in 1996 and Item 7 was extracted as a result, because its correlational value was found to be inadequate. The scale was implemented on the basis of 34 items; its Cronbach alpha coefficient was calculated as 0.89 (National Institute for Clinical Excellence, 2012). In the present study, the 34-item scale was used and the Cronbach alpha reliability coefficient was found to be 0.97. A high level of total points on the Self-care Agency Scale indicates the individual with diabetes mellitus is adequately able to act independently in self-management.
Analysis
In this correlational and descriptive study, the SPSS 16.00 statical programme was used and the Chi-square test was applied to determine whether there were differences between the three groups in terms of descriptive characteristics. Variance analysis was used to assess the effect of the mode of diabetes education on the level of knowledge, self-care agency, A1c and BMI. Tukey's HSD test was applied to determine which variable was responsible for the effect. The degree to which the variables influenced the results was evaluated through multiple regression analysis. The reliability interval used in the evaluation of the results was 95%. There was no difference in the outcomes according to the different types of diabetes.
Ethical Considerations
The consent form was approved and official written permission was obtained for the study from the Dokuz Eylül University ethics committees and the Aegean University Hospital ethics committees. The patients who agreed to participate after being informed by the researchers of the purpose and methodology of the study were given a consent form to sign and asked to respond to the questions in the questionnaire.
Results
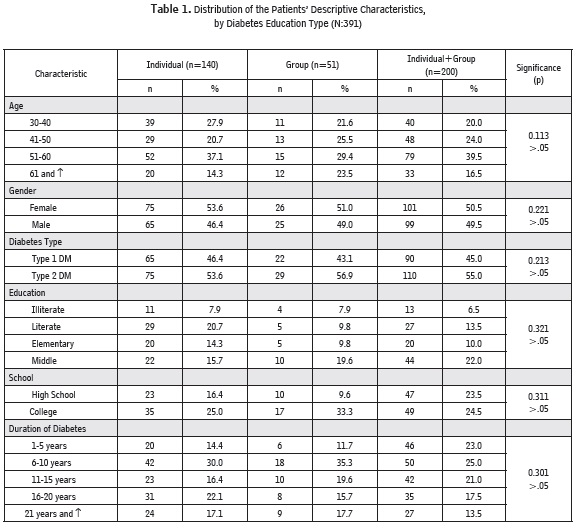
The corelational, descriptive characteristics of the study population comprising the sample; namely, age, gender, diabetes type, education, duration of diabetes (years) and the type of diabetes education the patient had received, are summarized in Table 1. Out of the 391 diabetics in the sample, it was found that 140 (35.8%) had received individual education, 51 (13.04%) had received group education and 200 (51.1%) had attended both individual and group education sessions. These results show us that increasing a patient's educational level also increases his/ her commitment to diabetes education. The descriptive characteristics of these subjects did not differ significantly according to the three types of education (p>0.05).
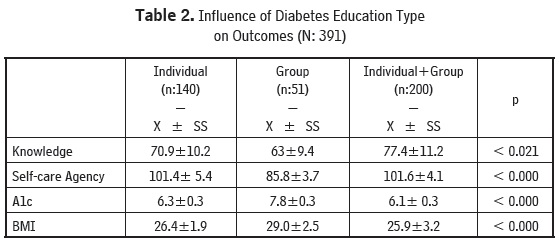
The study population's diabetes knowledge, A1c, BMI and self-care agency values are shown in Table 2, according to the type of education received. The values for level of knowledge, A1c, BMI and self-care agency differed according to the type of education received. This difference proved to be be statistically significant (p = 0.021, knowledge; p = 0.000, self care agency, A1c and BMI). Using the Turkish HSD test, it was found the difference stemmed from the group sessions;those receiving group education had lower values for knowledge and self-care agency,A1c and BMI compared to the other two groups.
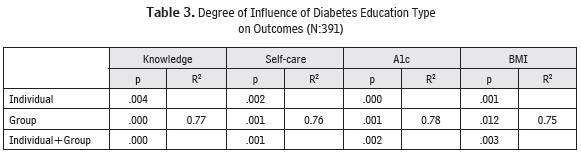
The degree to which education type influences knowledge, A1c, BMI and self-care agency is shown in Table 3. The multiple regression analysis carried out to determine the degree of influence demonstrated the method of education was able to affect the level of knowledge by 77%, self-care agency by 76%, A1c by 78% and BMI by 75% (R2: 0.77, R2 :0.76, R2 : 0.78, R2 : 0.75).
Discussion
This study showed the patients who received group education had lower values for diabetes knowledge, A1c, BMI and self-care agency than the other two groups, while the patients who had received both individual and group education had the highest values. In other words, it can be said that group education alone was inadequate and individual education by itself was also less effective than both individual and group education combined.
In studies where the type of education was analyzed in the literature, two outcomes were reported. Either the effects of individual and group education on final results have been found to be similar, or group education has been determined as being comparatively more effective. In three back-to-back reviews, it was stated that both individual and group education were effective in teaching lifestyle changes and skills and in ensuring glycemic control, but that each method has its own advantages and disadvantages (Norris, Lau, Smith & et al., 2002; Mensing & Norris, 2003; Funnell, Brown, Childs& et.al., 2007). In one review, group education was found to be more effective (Mannucci, Pala & Rotella, 2005). In addition to these reviews, studies conducted in later years also show group education is either more effective compared to an individual approach or the effects of individual and group sessions on results are similar (Uttech, 2006; Kulzer, Hermanns, Reinecker & et al., 2007; International Diabetes Federation, 2012). However, the result obtained in our study is different from the literature and is to the disadvantage of group education. Our study determined group education was less effective than individual education in improving the outcome for individuals with diabetes. Only Uttech's study refers to a result that is similar to ours. Uttech stated group education has no influence on self-adequacy (Jarvinen, Juurinen, Alvarsson & et al., 2007). The reason for this may be the difference in research methodologies. All the studies comparing the effects of diabetes education methods on outcomes are experimental and most focus on the effectiveness of group education versus individual education. Among these studies, ours is the only one that is not experimental. The study carried out in this case took place at two centers where both individual and group education were being delivered to patients in an effort to develop self-management skills in persons with diabetes. Group education at these centers sometimes involved groups of more than 20 patients. This may have been a factor in reducing the effectiveness of group education. However, our study showed the effectiveness of both individual and group education was decidedly more pronounced compared to individual or group education by itself. This leads one to think that individual and group education support and complement each other. The fact that the patient in an individual session is able to express him/herself more freely, understand better what the health professional is teaching and reach an effective outcome may lead to an awareness at the individual level that facilitates a more effective response in group education.
At the same time, the theory of adult learning should not be overlooked (Baumgartner, Lee, Birden & et al., 2003). According to that theory, an adult learns when there is a need to learn, problem-solving is more important than content, every individual's style of learning is different, and planning and evaluation must be carried out effectively (American Association Of Clinical Endocrinologists Guideline, 2012). The theory suggests that perhaps patients should be given a choice of more than one learning environment to meet their learning needs.
The continuity of education is also an important factor in bringing about changes in knowledge and behavior (Pinar,1999; National Institute for Clinical Excellence, 2012). In our study, we were not able to learn how many individual and group sessions each patient had attended. Were this possible, the fact that diabetic patients receiving both individual and group education had better outcomes could have been tied to their having attended a greater number of individual or group sessions. Not being able to clarify this point was a weakness in our study.
However, the data collected are supported by the guide published by the National Institute for Clinical Excellence, in which it is emphasized that a combination of individual and group education has a positive effect on patient results (Baumgartner, Lee, Birden & et al.,2003). The ADA 2012 Guidebook also supports this view (American Diabates Association, 2012).
Conclusion
At the end of this study, it was established that individual or group education was not sufficient, by itself, to improve the outcome for a person with diabetes. According to the research results, the recommendation might be to have every patient diagnosed with diabetes attend individual and group education sessions. Nurses can use both individual and group education to get the best results at clinics. It might be appropriate to conduct studies on education methods, outcomes and cost at the place of implementation, while continuing with experimental studies
Relevance to clinical practice: Diabetes education is effective when it comes to improving clinical outcomes, at least in the short-term. Individual and group diabetes education is a guide for diabetes nurses at clincs. This education could make it easier for nurses in clinical situations to follow-up on patients with diabetes.
Limitations of the study: One limitation obeys the fact that dataon the patients who were excluded from the sample could not be reviewed due to a lack of information in their files.
Conflict of interest
The authors stated no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. American Association of Clinical Endocrinologists Guideline (AACE, 2012). (Access: 25.03.2013). Available at: http://www.aace.com
2. American Diabates Association (ADA,2012). Standarts of Medical Care in Diabetes. http://www.diabetes.org (Access: 25.03.2013).
3. Baumgartner LM, Lee MY, Birden S, et al. (2003). Adult learning theory: a primer information series, center on education and training for employment. Ohio State University. ERIC Publications. (Access: 25.03.2013). Available at: http://www.cete.org/acve/docs/theory.pdf
4. Bilir M, & Çagdas Y. (2004). Yetiskin egitimi liderlerinden eduard christian lindeman yasami, egitim görüsü ve hizmetleri. Ankara University. Journal of Faculty of Educational Sciences, 37: 15-25. (in Turkish).
5. Deakin T, McShane C, Cade JE, et al. (2005). Group based self-management education in adults with type 2 diabetes mellitus (Review). Cochrane Database Systematic Review, 2.
6. Funnell MM, Brown TL, Childs BP, Haas LB, Hosey GM, Jensen B, Maryniuk M, Peyrot M, Piette JD, Reader D, Siminerio LM, Weinger K, Weiss MA. (2007). National standards for diabetes self-management education. Diabetes Care, 30: 1630-1637.
7. International Diabetes Federation (IDF, 2012). Clinical guidelines task force. Global gudeline for type 2 diabetes. Brussels: International Diabetes Federation. (Access: 25.03.2013). Available at: http://www.idf.org/webdata/docs/IDF%20GGT2D.pdf
8. International Diabetes Federation Diabetes Atlas. (2011). Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Prac, Dec; 94(3):311-21.
9. Jarvinen HY, Juurinen L, Alvarsson M, et al. (2007).Initiate insulin by aggressive titration and education (INITIATE): A randomized study to compare initiation of insulin combination therapy in type 2 diabetic patients individually and in groups. Diabetes Care, 30: 1364-1369.
10. Kearney BY, Fleisher BJ. (1979). Development of an instrument to measure exercise of self-care agency. Res. Nurs Health, 22: 25-34.
11. Kulzer B, Hermanns N, Reinecker H, et al. (2007). Effects of self-management training in Type 2 diabetes: a randomized, prospective trial. Diabetic Medicine, 24: 415-423.
12. Mannucci E, Pala L, Rotella CM. (2005). Long-term interactive group education for type 1 diabetic patients. Acta Diabetologia, 42: 1-6.
13. Medicare Program. (2012). Health care finance administration, rules and regulations. Federal Register, 65: 83129-83154.
14. Mensing CR, Norris SL. (2003). Group education in diabetes: Effectiveness and implementation. Diabetes Spectrum,16: 96-103.
15. Nahcivan N. (1993). Saglikli gençlerde özbakim gücü ve aile ortaminin etkileri. Doctorate Thesis, Istanbul Üniversitesi, 64-66. (in Turkish).
16. National Institute for Clinical Excellence (NICE, 2012). Guidance on the use of patient- education models for diabetes. (Access: 25.03.2013). Available at: http://www.formulary.cht.nhs.uk/Guidelines/NICE/060_Pt_Ed_Diabetes.htm
17. Norris SL, Engelgau MM, Narayan KMV. (2001). Effectiveness of self-management training in type 2 diabetes: a systematic review of randomized control trials. Diabetes Care, 24: 561-587.
18. Norris SL, Lau J, Smith SJ, et al. (2002). Self-management education for adults with type 2 diabetes: a meta-analysis of the effect on glycemic control. Diabetes Care, 25: 1159- 1171.
19. Pinar R. (1999). Diabetes mellituslu hastalarda özbakim gücü ve özbakim gücünü etkileyen sosyodemografik faktörlerin incelenmesi. Türk Diyabet Yilligi,11: 1248-2579. (in Turkish).
20. Rickheim PL, Weaver TW, Flader JL, et al.(2002). Assessment of group versus individual diabetes education. Diabetes Care, 25: 269-274.
21. Uttech CJ. (2006) (Counseler: Edelstein, Jan). Survey of diabetes self-efficacy for individuals newly diagnosed with type two diabetes before and after empowerment group education. Marian College of Fond du Lac, AAT 1440799.68. (Access: 25.03.2013). Available at: http://proquest.umi.com/pqdweb
22. Wild S, Roglic G, Gren A, et al. (2004). Global prevalence of diabetes estimates for the year 2000 and projections for 2030. Diabetes Care, 27: 1047-1053.
23. Zrebiec J. (2003). Tips for running a successful group. Diabetes Spectrum, 16:108-110.