Childbirth and Postpartum Period Fear in Pregnant Women and the Affecting Factors
El miedo del parto y puerperio en mujeres embarazadas y los factores que lo afectan
O medo do parto e do puerpério em gestantes e os fatores que as afetam
Recibido: 01 de octubre de 2014
Enviado a pares: 23 de noviembre de 2014
Aceptado por pares: 24 de noviembre de 2015
Aprobado: 02 de diciembre de 2015
Nuray Egelioğlu Cetişli1
Zubeyde Denizci Zirek2
Fatma Bakilan Abali3
1 Izmir Katip Celebi University, Faculty of Health Sciences, Izmir, Turkey.
nurayegelioglu@gmail.com
2 Izmir Katip Celebi University Atatürk Education and Research Hospital, Izmir, Turkey.
zubeydedenizci@yahoo.com
3 Izmir Katip Celebi University Atatürk Education and Research Hospital, Izmir, Turkey.
fatosabali@hotmail.com
Para citar este artículo / To reference this article / Para citar este artigo
Egelioğlu Cetişli N., Denizci Zirek Z. Y Bakilan Abali F. Childbirth and postpartum period fear in pregnant women and the affecting factors. Aquichan. 2016;16(1):32-42. DOI: 10.5294/aqui.2016.16.1.5
|
ABSTRACT Objective: The aim of this study was to identify the anxiety pregnant women feel about childbirth and the postpartum period and to determine the affecting factors. Methods: A descriptive design was used in the study, which was conducted with pregnant women at two obstetric polyclinics of a university hospital in Turkey from January 2014 to July 2014. The population consisted of 143 pregnant women. The data were collected using an individual identification form and the Fear Childbirth and Postpartum Anxiety Scale. The percentage, Kruskall Wallis, Mann-Whitney U and Independent Sample t tests were used to evaluate the differences between the variables. Results: The results of the study reveal that pregnant women are quite fearful of childbirth and the postpartum period. Conclusions: It is necessary to decrease fear of childbirth, because of its negative effects. KEYWORDS Pregnancy; labor; postpartum period; nursing care (Source: DeCS, BIREME). |
RESUMEN Objetivo: el objetivo de este estudio fue determinar la ansiedad de las mujeres embarazadas en relación con el parto y el puerperio y determinar los factores que las afectan. Métodos: se utilizó un diseño descriptivo y el estudio se llevó a cabo con un grupo de mujeres embarazadas en dos policlínicas obstétricas de un hospital universitario en Turquía desde enero de 2014 hasta julio de 2014. La población estuvo constituida por 143 mujeres embarazadas. Los datos fueron recolectados a través de un formulario de identificación individual y la Escala de Miedo al Parto y el Puerperio. Las pruebas de porcentaje, Kruskall Wallis, U de Mann-Whitney y la prueba t para muestras independientes se utilizaron para evaluar las diferencias entre las variables. Resultados: los resultados del estudio revelaron que las mujeres embarazadas tienen un alto nivel de miedo con respecto al parto y el puerperio. Conclusiones: es necesario disminuir ese miedo debido a sus efectos negativos. PALABRAS CLAVE Embarazo; parto; puerperio; cuidados de enfermería (Fuente: DeCS, BIREME). |
RESUMO Objetivo: o objetivo deste estudo foi determinar a ansiedade das gestantes quanto ao parto e ao puerperio e determinar os fatores que as afetam. Métodos: utilizou-se um desenho descritivo, e o estudo foi realizado com um grupo de gestantes em duas policlínicas obstétricas de um hospital universitário na Turquia, de janeiro a julho de 2014. A população esteve constituída por 143 gestantes. Os dados foram coletados por meio de um formulário de identificação individual e pela Escala de Medo do Parto e do Puerpério. Os testes de porcentagem, Kruskall Wallis, U de Mann-Whitney e o teste-t para amostras independentes, foram utilizados para avaliar as diferenças entre as variáveis. Resultados: os resultados do estudo revelaram que as gestantes têm um alto nível de medo do parto e do puerpério. Conclusões: é necessário diminuir esse medo devido a seus efeitos negativos. PALAVRAS-CHAVE Gestação; parto; puerpério; cuidados de enfermagem (Fonte: DeCS, BIREME). |
Introduction
Pregnancy is an important transition period for women moving into motherhood. It also is a time when women might experience a number of physiological and psychological changes. Today, childbirth is thought to be a frightening matter requiring medical attention, rather than a normal condition (1, 2). The literature contains many studies on worries and anxiety about childbirth. The fears of women identified in these studies were pain, panic, sense of failure, losing control, injury to the child and the mother, emergency cesarean section, excessive bleeding, residual part of the placenta, and the development of complications during birth, such as hypertension, permanent damage to the child, episiotomy and death of mother or her child. The literature also shows that women fear damage to the perineum area, adverse effects on sexual life, the screams of the medical staff, failure at birth or insufficient support (1-21). As for the postpartum period, the fears of pregnant women were identified as being centered on infant care and the adverse effects it might have on their marriage and family life. During the third trimester in particular, as the birth time approaches, increasing anxiety can cause adverse effects and pain at birth, decreased pain tolerance, a longer birth process, more need for analgesics, a rise in arbitrary demand for caesarean sections, and an increase in the risk of psychological disorders during the postpartum period (22, 23).
Birth anxiety can be seen in many pregnant women because of the violence in the process of birth. Therefore, the medical staff should be aware of the emotional changes and fears a woman can undergo during pregnancy, childbirth and the postpartum period. Moreover, to reduce anxiety, they should be able to provide training and coaching on the process of pregnancy and birth. Nurses, who are at the center of the team of health professionals, should continually evaluate the process of normal and/or abnormal pregnancy as it occurs during the birth process. According to the Roy Adaptation Model, nurses are able to identify and determine appropriate/inappropriate behavior during this natural stage of human developmental from pregnancy to childbirth (15, 20, 27). The types of behavior to be identified are different in the development of a normal or abnormal process with respect to post conception, gestation, pregnancy complications, live birth and/or fetal death during the natural process of childbirth. Also, nurses are able to determine the stimulant factors causing positive behavior during changes in labor. To plan the nursing care process, to provide appropriate care services and to reduce the fears of pregnant women, it is important to identify the affecting factors and, thus, reduce complications at the time of birth (1, 7-12, 20, 25, 27, 28). This study was conducted to determine the anxiety pregnant women experience during childbirth and the postpartum period, and to determine the factors affecting that fear.
Materials and Methods
Design
This descriptive study was carried out at two obstetric polyclinics of a university hospital in Izmir, Turkey. The working hours of the obstetric polyclinics where the study was conducted were from 8:00 a.m. to 5:00 p.m. The number of working days was five per week.
Participants and Setting
The sample for this research consisted of 143 women between the ages of 18 and 45 who went to the university obstetric polyclinic for routine pregnancy check-ups during the period from January 2014 to July 2014. The pregnant women in this sample were in the 37th week of their pregnancy or more, had no risk factors or psychological problems, and each of them consented to take part in the study.
Data Collection
The data were collected by the researchers during a face-to-face interview with each pregnant woman before she was called in to see the doctor. The interview was conducted in a waiting room during a period of 15-20 minutes.
The individual identification form and the Fear of Childbirth and Postpartum Anxiety Scale (FFCP) were used to gather the data.
Measures
The individual identification form was created by the researchers on the basis of relevant literature. The form consisted of 13 questions designed to collect data on the socio-demographic and obstetric characteristics of the pregnant women.
The Fear of Childbirth and Postpartum Anxiety Scale (FCPP), the reliability and validity of which was approved (Cronbach alpha = 0.955) by Kitapçioğlu et al., has 61 questions and 10 factors (Kitapçioğlu et al., 2008). The FCPP is Likert-type and the scores are as follows: 1: Completely Disagree, 2: Disagree, 3: Not Sure, 4: Agree, 5: Completely Agree. In the scale, all the scores obtained from each factor are standardized before being summed up and divided by the factor number. Then, the total score on the scale is calculated. The resulting scores are evaluated as Very Low: 0.00-2.00, Low: 2.01-4.00, Medium: 4.01-6, High: 6.01-8.00 and Very High: 8.01-10.00 (11).
Analysis
For this descriptive study, SPSS 16.00 Statistical Software was used in the calculations to determine the demographic and obstetric characteristics of the pregnant women. The results are statistically significant at the level of p<0.05. The Kruskall Wallis, Mann-Whitney U, and Independent Sample t tests were used to evaluate the differences between the variables.
Ethical Considerations
The consent to conduct of this research was officially approved. A signed written document was issued by the Ethics Committee of the Izmir Katip Celebi University to perform the study. First, the pregnant women to be included in this study were informed about its purpose and methodology. Those who agreed to participate were given a consent form to be signed. Since they approved their participation by signing the form, they were asked to answer the research questionnaire.
Results
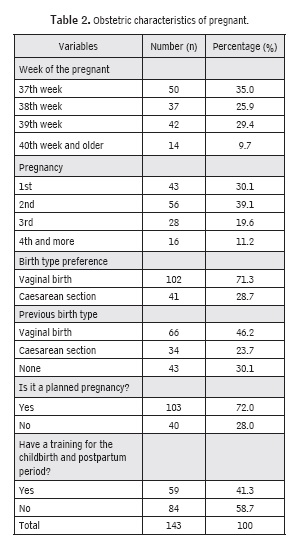
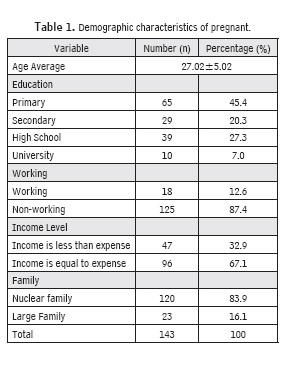
The demographic characteristics of the pregnant women are shown in Table 1. The average mean age of the participants was 27.02±5.02. In all, 45.4% were primary school graduates, 87.4% were housewives, 67.1% had an income equal to their expenses, and 83.4% had a nuclear family structure (Table 1). Moreover, 35.0% of the pregnant women in the sample were in their 37th week of pregnancy and 39.1% reported this was their second pregnancy; 71.3% were planning a vaginal birth, and 46.2% had a vaginal birth with their previous pregnancy. Finally, 72.0% reported this pregnancy as being planned and 58.7% received antenatal training for the birth and the postpartum period (Table 2).
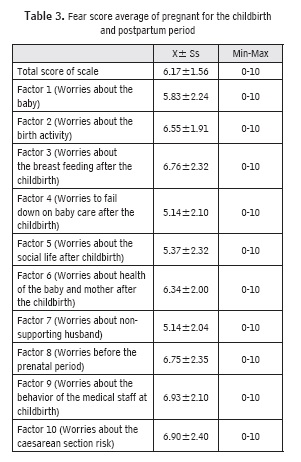
The average total score on the FCPP for the pregnant women was 6.17±1.56. The highest average subscale score for anxiety concerned the medical staff's behavior, at 6.93±2.10. Anxiety about a cesarean section comes next, with a score of 6.90±2.40. The average subscale score for anxiety over breast feeding was 6.76±2.32, while worries about the prenatal period had almost an equal score (6.75±2.35). Other average subscale scores for anxiety, in descending order, were about labor (6.55±1.91), health of the mother and baby after childbirth (6.34±2.00), the baby (5.83±2.24), social life after childbirth (5.37±2.32), insufficient postnatal infant care (5.14±2.10) and, finally, lack of support from the husband (5.14±2.04). As for the total score averages, what the pregnant women feared the most was poor behavior by medical staff at the birth, followed by the risk of cesarean section, breastfeeding, the prenatal period, labor and postnatal infant care (Table 3).
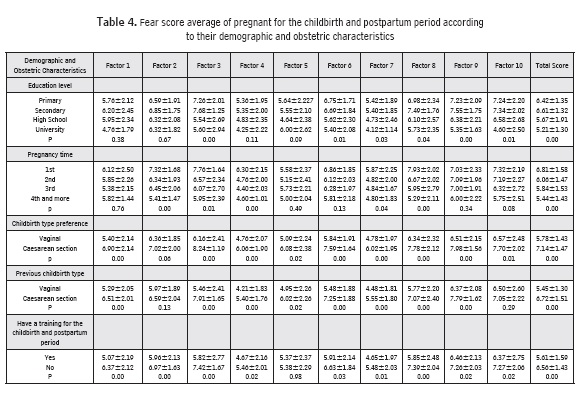
When the authors checked the relationship between the average scores on the anxiety scale and the demographic and obstetric characteristics, a statistically significant difference was identified with respect to level of education, week of pregnancy, number of pregnancies, preferred mode of childbirth, previous mode of childbirth, and training for the antenatal and postpartum period. The lowest anxiety scores were for the participants who were university graduates, had four or more pregnancies, preferred vaginal birth, underwent a vaginal birth in their previous pregnancy, and had training for the antenatal and postpartum period (Table 4).
Discussion
In many cultures, pregnancy is acknowledged as a natural and normal occurrence. Anxiety about birth is seen frequently and causes several severe problems during childbirth (1-8, 12-15, 21). In this study, it was determined that pregnant women have a high level of anxiety about childbirth and the postpartum period, and worry about the negative behavior of the medical staff during labor. Furthermore, pregnant women fear the risk of a caesarean section, the prenatal period and labor. The study also showed pregnant women fear they will fail at breast feeding and postnatal infant care. Melender (2001) conducted a study to determine the fear factors during pregnancy and at birth, their causes and formations. In that study, the results showed the fear factors concerned the health of the infant and the mother, the behavior of the medical staff, caesarean section, and the family after labor (13).
Sercekus and Okumus (2009) conducted a study on nulliparous pregnant women and reported that labor and poor behavior on the part of the staff cause birth fear (20). A medical staff member who is well-informed and supportive of the birth process during the intrapartum period is very important to inspiring confidence and support for the pregnant woman and the family, and also can be highly effective in providing basic information (1-5, 7-10). Sjögrenet et al. (1997) reported that pregnant women who were supported by the medical staff at the clinic felt more self-sufficient, their satisfaction ratio increased, and they had less fear of childbirth (22). Nurses, who spend the most time with pregnant women in the intrapartum unit, should be aware of the stress diagnosis for women in birth activity; they also should be conscious of their physical and psychological needs, and help them to manage labor and to ensure the birth concludes with a healthy mother and baby. In this study, the fear factors in the prenatal period and during childbirth were identified as focused on being unable to go to the hospital in time, being alone when labor pains begin, early loss of amniotic fluid, loss of control during labor, prolonged labor, and loss or damage to the baby.
Fear causes severe problems and also results in an increased demand for caesarean sections. The World Health Organization (WHO, 2015) says the ratio of caesarean sections should be less than 15% (26). Unfortunately, the caesarean ratio in Turkey is higher than WHO's recommendation. According to the Turkey Demographic and Health Survey (2013), the caesarean ratio in Turkey was 48% (24). The opinion of women regarding a caesarean section and a vaginal birth differs among the different cultures (1-8, 12-15). Studies conducted on the opinions of women report the following as the reasons why women prefer vaginal delivery: birth is regarded as a normal condition, the feeling of being in control of oneself, the experience of vaginal birth, shorter recovery time and earlier discharge from the hospital, lower complication ratios, fear of anesthesia and surgery, the sense of being safer for the mother, improved affection for the infant, less pain in the postpartum period, "better for health", being able to breastfeed directly, considered trustworthy, "normal birth is best," and the husband's support for normal birth (13-16, 18, 21, 23, 25, 27, 28). The researchers reported a higher ratio of maternal mortality, postpartum hemorrhage, uterine rupture and infection. They also indicated that urinary area and placenta previa damage in the next pregnancy, still birth, spontaneous abortion and the risk of ectopic pregnancy was higher (17, 25, 27, 28).
In this study, it was found that women who prefer vaginal birth and who experienced a vaginal birth in their previous pregnancy had less fear of birth and the postpartum period than women who preferred and experienced a caesarean section. The belief in Turkey is that labor experienced during childbirth enhances the emotions and the body is cleansed by bleeding at birth. There is also the feeling that it helps to recover from certain gynecological complaints (23, 27). Pregnant women reported that having a more active role in childbirth and directly experiencing birth affects their feelings and increases bonding with the infant. It is a common belief that experiencing more pain results in a rich feeling of motherhood (3, 23, 27).
The results of this study showed the women were extremely anxious about infant care and breastfeeding after birth. For Turkish women, recovering quickly after giving birth and taking care of the infant as soon as possible are very important (19, 20, 23). This social point of view for the mother was considered, in this study, to be the reason for anxiety about inability in infant care and breast feeding during the postpartum period. Although there is some support from the family and help for the mother in terms of child care, it is important for women to look after and breast feed their infants themselves (18-20, 23).
Haines et al. (2011) reported that women who are primiparous and have less education experience higher birth fear levels (8). Alehagen et al. (2006) conducted a study with 35 primipara and 39 multipara women, and compared birth fear between the two groups. They reported that primipara pregnant women have more fear compared to multipara pregnant women (2).
The results in this study were consistent with the literature (4-6). Not having experience with birth, ambiguous feelings and lack of knowledge were thought to be the reason for the high level of fear among primipara pregnant women. The study also showed the pregnant women who had no training for childbirth and the postpartum period experienced more birth fears compared to the pregnant women who had training. This result is consistent with other studies found in the literature. For example, Cosar and Demirci (2012) conducted a study to analyze the effect of birth preparatory training on the perception of birth and adaptation to it. The women in the group who received training experienced less fear of birth (3). Haines et al. (2011) reported that training and care given in the antenatal period is an important factor in fear of birth and was shown to decrease the level of birth fear (8).
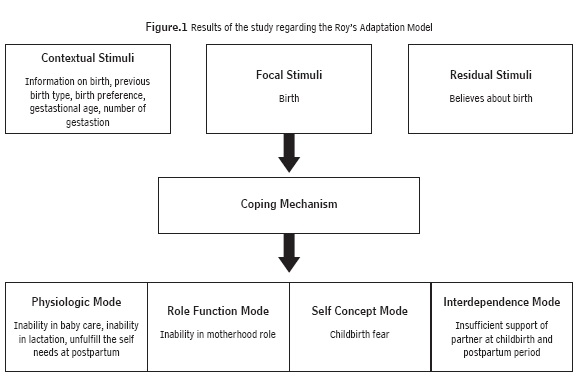
Finally, the results of this study were analyzed with respect to the Adaptation Model. The analysis showed that inappropriate behavior in adaptation area four causes birth fear (Figure 1) (19, 20). Identifying pregnant woman's fears and expectations about childbirth is very important for nurses, if they are to provide effective nursing care.
Conclusion
It was determined in this study that pregnant women have high levels of anxiety about childbirth and the postpartum period. The results showed the highest level of fear concerns the behavior of the medical staff. The other fear factors that were identified involve caesarean sections, antenatal labor, the birth itself, breast feeding and infant care after birth. The results also revealed that pregnant women who were primiparas, poorly educated and had a caesarean section in a previous birth or prefer a caesarean section experienced a higher level fear.
Recommendations for Practice
The results of this study suggest that broadening prenatal training classes and conducting training to develop the nurse's awareness will help to lower the level of fear and anxiety about childbirth and the postpartum period, and will contribute to healthy birth activity and effective preparation for birth, in conjunction with woman's partner. It also will help to raise the couple's awareness about birth.
Conflict of Interest
The authors stated no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Adams SS, Eberhard-Gran M, Eskild A. Fear of childbirth and duration of labour: A study of 2206 women with intended vaginal delivery. BJOG: An International Journal of Obstetrics & Gynaecology. 2012; 119: 1238-1246.
2. Alehagen S, Wijma B, Wijma K. Fear of childbirth before, during, and after childbirth. Acta Obstetrica et Gynecologica Scandinavica.2006;85(1):56-62.
3. Cosar F, Demirci N. The effect of childbirth education classes based on the philosophy of Lamaze on the perception and orientation to labour process. Süleyman Demirel University Journal of Health Science. 2012; 3(1):18-30.
4. Eriksson C, Jansson L, Hamberg K. Women's experiences of intense fear related to childbirth investigated in a Swedish qualitative study. Midwifery. 2006; 22(3): 240-248.
5. Fenwick J, Gamble J, Nathan E, Bayes S, Hauck Y. Pre- and postpartum levels of childbirth fear and the relationship to birth outcomes in a cohort of Australian women. Journal of Clinical Nursing. 2009; 18(5):667-677.
6. Fisher C, Hauck Y, Fenwick J. How social context impacts on women's fears of childbirth: A Western Australian example. Social Sciences Medicine. 2006; 63(1): 64-75.
7. Fuglenes D, Aas E, Botten G, Oian P, Kristiansen IS. Why do some pregnant women prefer cesarean? The influence of parity, delivery experiences, and fear. American Journal of Obstetrics Gynecology. 2011; 205(45): 1-9.
8. Haines H, Pallant JF, Karlstrom A, Hildingsson I. Cross-cultural comparison of levels of childbirth-related fear in an Australian and Swedish sample. Midwifery. 2011; 27(4): 560-567.
9. Haines HM, Rubertsson C, Pallant JF. Hildingsson I. The influence of women's fear, attitudes and beliefs of childbirth on mode and experience of birth. BMC Pregnancy and Childbirth. 2012; 12: 55.
10. Karlstrom A, Nystedt A, Hildingsson I. A comparative study of the experience of childbirth between women who preferred and had a caesarean section and women who preferred and had a vaginal birth. Sexual & Reproductive Healthcare. 2011; 2(3): 93-99.
11. Kitapçioğlu G, Yanikkerem E, Sevil Ü,Yüksel D. Fear of childbirth and the postpartum period: A scale development and validation study. Journal of Adnan Menderes University Medical Faculty. 2008; 9(1):47-54.
12. Laursen M, Johansen C, Hedegaarda M. Fear of childbirth and risk for birth complications in nulliparous women in the Danish National Birth Cohort. BJOG: An International Journal of Obstetrics & Gynaecology. 2009; 116(10): 1350-1355.
13. Melender HL. Experiences of fears associated with pregnancy and childbirth: A study of 329 pregnant women. Birth. 2002; 29(2): 101-111.
14. Nilsson C, Lundgren I. Women's lived experience of fear of childbirth. Midwifery. 2009; 25(2): 1-9.
15. Nilsson C, Lundgren I, Karlstrom A, Hildingsson I. Self-reported fear of childbirth and its association with women's birth experience and mode of delivery: A longitudinal population-based study. Women and Birth. 2012; 25(3): 114-121.
16. Rouhe H, Salmela-Aro K, Halmesmaki E, Saisto T. Fear of childbirth according to parity, gestational age, and obstetric history. BJOG: An International Journal of Obstetrics & Gynaecology. 2009; 116(1):67-73.
17. Saisto T, Salmela-Aro K, Nurmi JE, Könönen T, Halmesmaki E. A Randomized Controlled Trial of Intervention in Fear of Childbirth. Obstetrics and Gynecology. 2001; 98(5): 820-826.
18. Sayiner FD, Özerdogan N, Giray S, Özdemir E, Savci A. Identifying the women's choice of delivery methods and the factors that affect them. Perinatal Journal. 2009; 17(3): 104-112.
19. Serçekuş P. Intervention for fear of childbirth: Hypnobirthing. TAF Preventive Medicine Bulletin. 2011; 10(2): 239-242.
20. Serçekuş P, Okumuş H. Fears associated with childbirth among nulliparous women in Turkey. Midwifery. 2009; 25(2): 155-162.
21. Spice K, Jones SL, Hadjistavropoulos HD, Kowalyk K, Stewart SH. Prenatal fear of childbirth and anxiety sensitivity. Journal of Psychosomatic Obstetrics & Gynecology.2009; 30(3): 168-174.
22. Sjögren B. Reasons for anxiety about childbirth in 100 pregnant women. Journal of Psychosomatic Obstetrics & Gynecology.1997; 18(4): 266- 272.
23. Taşçi Duran E, Ünsal Atan Ş. Qualitative analysis of perspectives of woman about cessation section/vaginal delivery. Genel Tip Dergisi. 2011; 21(3): 83-88.
24. TDHS. Turkey Demographic and Health Survey, 2013. Retrieved May 3, 2014 (http://www.hips.hacettepe.edu.tr/eng/TDHS_2013_main.report.pdf)
25. Waldenstrom U, Hildingsson U, Ryding E. Antenatal fear of childbirth and its association with subsequent caesarean section and experience of childbirth. BJOG: An International Journal of Obstetrics & Gynaecology. 2006; 113(6):638-646.
26. WHO statement on caesarean section rates, 2015. (http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/cs-statement/en/)
27. Yaşar Ö, Şahin F, Coşar E, Nadirgil-Köken G, Cevrioğlu AS. Birth method choices of primiparous women and the factors which have an effect on these choices. Turkiye Klinikleri Journal of Gynecology and Obstetrics. 2007; 17(6): 414-420.
28. Zar M, Wijma K, Wijma B. Pre - and postpartum fear of childbirth in nulliparous and parous women. Scandinavian Journal of Behaviour Therapy. 2001; 30(30):75-84.