Articles
CarlaChacón Valera 1
Maria Bartolomé Regué 2
Sergi Font Ritort 3
Esther Cabrera Torres 4
1 ![]() orcid.org/0000-0001-8524-6189. Escuela Superior de Ciencias de la Salud, Universidad Pompeu Fabra, Spain. cchacon@escs.tecnocampus.cat
orcid.org/0000-0001-8524-6189. Escuela Superior de Ciencias de la Salud, Universidad Pompeu Fabra, Spain. cchacon@escs.tecnocampus.cat
2 ![]() orcid.org/0000-0002-9802-3811. Consorci Sanitari del
Maresme, Spain. mbartolome@csdm.cat
orcid.org/0000-0002-9802-3811. Consorci Sanitari del
Maresme, Spain. mbartolome@csdm.cat
3 ![]() orcid.org/0000-0003-0056-0457. Consorci Sanitari del Maresme, Spain. sfont@csdm.cat
orcid.org/0000-0003-0056-0457. Consorci Sanitari del Maresme, Spain. sfont@csdm.cat
4 ![]() orcid.org/0000-0002-7353-0542. Escuela Superior de Ciencias de la Salud, Universidad Pompeu Fabra, Spain. ecabrera@tecnocampus.cat
orcid.org/0000-0002-7353-0542. Escuela Superior de Ciencias de la Salud, Universidad Pompeu Fabra, Spain. ecabrera@tecnocampus.cat
Received:23/10/2018
Sent to peers: 05/11/2018
Approved: 06/12/2018
Accepted: 10/01/2019
10.5294/aqui.2019.19.1.5
The topic: Promotion and prevention.
Contribution to the discipline: The increasing population aging brings up to health professionals, especially to community nursing, the need to know and develop the factors that have an impact on the positive development and well-being of elderly people. The present study provides a faithful picture of the training needs and interests perceived by the elderly adults in Mataró. From these results, nursing can plan interventions which can be implemented from primary care centers, based on the interests of the target population, with a greater guarantee that they will improve the follow-up of health and quality of life guidelines to cope with aging in a healthier way.
To reference this article / Para citar este artículo / Para citar este artigo: Chacón C, Bartolomé M, Font S, Cabrera E. Cómo afrontar el envejecimiento de forma saludable: cambios y oportunidades. Aquichan; 19(1): e1915. DOI: 10.5294/aqui.2019.19.1.5
|
ABSTRACT Objective: To know the socio-demographic
characteristics of the elderly adults (60-70 years), of the population of
Mataró (Barcelona), and their relationship with the knowledge degree and
training needs perceived to face a healthy aging. KEY WORDS (source Decs): Aging; retirement; health; habits; healthy lifestyle; training; knowledge. |
RESUMEN Objetivo: conocer las características sociodemográficas de las
personas adultas mayores (60-70 años) de la población de Mataró (Barcelona) y
su relación con el grado de conocimientos y las necesidades formativas
percibidas para afrontar un envejecimiento saludable. PALABRAS CLAVE (fuente: DeCS): Envejecimiento; jubilación; salud; hábitos; estilo de vida saludable; capacitación; conocimiento. |
RESUMO Objetivo: conhecer as características sociodemográficas das
pessoas idosas (60-70 anos) da população de Mataró (Barcelona) e sua relação
com o grau de conhecimentos e com as necessidades formativas percebidas para
encarar um envelhecimento saudável. Palavras-chave (fonte: DeCS): Envelhecimento; aposentadoria; saúde; hábitos; estilo de vida saudável; capacitaçao; conhecimento. |
Introduction
Aging is a physiological transformation process which is inherent to the human being and it evolves differently on each person. It is considered an important change in people’s lives because it changes their daily routines and affects their own perception and their health-related behaviours (1, 2). The world is undergoing a demographic transformation: The life expectancy increase and the fertility rate decrease are causing an inversion of the population pyramid (2, 3). Currently, the Spanish society reveals one of the highest life expectancies in the world: 82.87 years (4).
During aging, dependency rates, disability and chronic diseases increase which causes a greater expenditure of social and health resources (5). In addition to the physical consequences, there are changes that can significantly influence the quality of life of elderly people, such as the retirement.
Retirement marks a turning point in people’s lives since it constitutes a transition that impels them to assume a new role in life. Despite this, many people find themselves immersed in this stage without having considered its meaning or the best way to cope with it (6, 7). Retirement challenges people to learn how to spend, satisfactorily, meaningfully and healthily, the time they have (8). Therefore, this moment is an ideal space to provide elderly adults (9) with intervention tools that allow them a good aging process (10).
Healthy aging is based on promoting and maintaining functional capacity that allows well-being during old age (2). However, a high percentage of people start this stage assuming excessive burdens that can harm their health and life quality (11, 12, 13): On one hand, the parents and grandchildren’s care and, increasingly, the partner’s care (9, 10); on the other, the growing number of elderly people living on their own and taking care of themselves (11, 12). Facing this scenario, there is a need to make changes in our healthcare system, coordinating health services and social services to achieve a healthy aging in a comprehensive, effective and sustainable way.
Health professionals have the opportunity and responsibility to respond to this new situation by enhancing preventive work, especially, the primary care nursing professionals, who have the community health work assigned.
Assisting the elderly to plan their old age stage, taking into account tertiary prevention, functional loss situations, and autonomy that are generated by having a chronic disease, can help to promote a healthy aging (14, 15). There are many documented interventions generated from the nursing experience to promote healthy aging (16, 17), but, in our environment, there are no studies in which the description of the subjects that concern elderly people, or what they think it would be useful to know have been identified. This is what in our study we have defined as “training needs”.
The increasing on population’s aging that we are currently facing is exerting a great pressure on social and health system (18, 19). Therefore, it is necessary to know the needs of the elderly adults and find answers that allow them to maintain their autonomy, functional independence and quality of life as long as possible (20).
The principal aim of this study was to know the elderly socio-demographic characteristics (60-70 years), of the population of Mataró (Barcelona), and their relationship with the knowledge degree and training needs perceived to face a healthy aging.
Materials and methods
Study design
Descriptive cross-sectional observational study carried out in the primary care centers (CAP), Cirera-Molinos, Gatassa, Mataró-Centro, Riera, Ronda Cerdaña and Ronda Prim, from the city of Mataró (Barcelona), which covers a population of 124,280 inhabitants (19), of which 12,309 are between 60 and 70 years old (47 % men and 53 % women) (20). The study started in May 2016 and concluded in May 2017.
Population and sample
The study population was the elderly people from the city of Mataró. The inclusion criteria were: being between 60 and 70 years old, being registered in the city of Mataró and being able to answer the survey autonomously. The exclusion criteria were: being included in the home care program (ATDOM), being admitted to a social or residential centre or not understanding Catalan or Spanish.
The sample was selected by a randomized sampling from the population census assigned to each health centre, estimating to obtain a sample size of 300 people. For the sample size, a confidence level of 95 % was established, a matrix whose x-axis presented the power 80 to 95 was presented, and expected correlations between 0,1 and 0,5. A sample size of at least 244 subjects was calculated, with a power of 95 and an expected correlation of 0,1. The final number of subjects surveyed was 306.
The research team was responsible for contacting the selected people; each subject was asked to participate by a telephone call. In the case that the selected patient did not meet the inclusion criteria or did not want to participate in the study, the next one was chosen from the list, and so on.
Study variables
The main variables analysed were self-perceived knowledge degree and the training needs or interests, as well as the occupation of free time, the health status, the dose regular medication and the pathological background. The socio-demographic variables that were taken into account were age, sex, country of birth, marital status, residence neighbourhood, health reference centre, the maximum level of education accomplished, employment situation, occupation, family situation and approximate amount of monthly household income.
Measurement instruments
The Questionnaire on Healthy Ageing (QHA) was used for data collection, developed ad hoc by a team of experts in the field of Geriatrics and primary health care. The QHA is aimed at the young elder population (60-70 years) and consisted of 139 items. The questionnaire evaluated demographics (including age, sex, country of origin, level of education, employment status, marital status, family situation and income level), how they spend their leisure time (activities carried out on a regular basis, including taking care of the grandchildren, time dedicated to them and caring of an ill relative), health status (this included two items which make reference to general health status: one of them has five options Likert-type response option, the second item was a vertical Visual Analogue Scale (VAS) of 20 centimetres, measured in millimetres, ranging from 0, which would be the worst imaginable health state, to 100, referring to the best imaginable health state). In it, the individual had to mark the point on the vertical line that best reflected the assessment of his/her global health in that moment. It also included four more items on chronic diseases, common medicines, degree of autonomy and perception of ageing, management of new technologies (section which consists of four items with option of a dichotomous response) and, finally, the training and training needs (included 112 items with Likert-type answer with four options each).
The QHA measures six dimensions of knowledge and training needs: Health, social, spiritual, legal and economic, and leisure traits. In order to calculate the results by size, the items were codified from 0 to 3, where 0 meant “nothing”, 1 “a little”, 2 “quite a lot”, and 3 “a lot”.
The total of the items belonging to the same dimension were added up together, and then, divided by the maximum possible score within in it, and the total was multiplied by 10, so each dimension was scored from 0 to 10 to ease the measurements’ comprehension.
The first version of the QHA was monitored by a group of 14 persons who matched with the study inclusion criteria. All of them contributed with their comments about the questionnaire through a form. Taking this into account, as well as for its extension, it was determined that the questionnaire could not be done on the telephone, and this could be auto-administrated. The final version was validated by health professionals from the social ambit, as well as with the investigating team.
Data collect
The subjects went to different health centres of the city, arrenged by telephone from their health centre. The questionnaire was completed in a self-administered way and under the supervision of two members of the research team. The questionnaire was completed in groups of between 5 and 10 people. It lasted approximately 20 minutes.
Data analysis
A descriptive analysis of the data with central tendency and dispersion measures for the quantitative variables, and with frequency distribution for the qualitative ones was realized. The level of statistical significance was established at a p-value <0,05. The comparisons between categorical variables were realized by means of the Chi-square test, and the continuous ones, with T-Student or their nonparametric equivalents. The data was analysed through the statistical program SPSS Statistics Version 14.0.
Ethical considerations
The study was fulfilled in accordance with the articles pertaining to the Helsinki Declaration on ethical principles for medical research in humans, approved by the 64th World Medical Assembly in 2013. The permission to carry out this study (version 6 of 03/16/2016) was obtained from the Ethics Committee of Clinical research of the Maresme Health Consortium and the University Institute for Research in Primary Care (IDIAP Jordi Gol). All the individuals participated voluntarily, and they informed about their consent for the study: They received an informative document explaining the objectives of the study and in what it consisted of.
Results
The data from a total of 306 subjects was obtained: The 52.1 % of them were men, and the 47,9 % women, with an average age of 64,4 years old (DS ± 3,19). The 77,6 % were married or maintained a relationship, the 12,5 % lived on their own, and the 28 % was taking care of an ill person, generally their parents. The 21 % didn’t have studies, and on the other hand, the 78 % had studies (primary studies [52 %]) or secondary studies/high school [26 %]). The digital alphabetization resulted to be majority on the positive side, as a 62,8 % of the participants affirmed to have skills on internet. As far as their labour situation, the 81,10 % were retired; the 65,60 % spend their time on, for example, sports or dancing (48,8 %), volunteering (20,8 %), arts or music (8,9 %), and more. Despite that, the 19,0 % was taking care of their grandchildren as the only activity. The 56,5 % of the participants was in good health and reflected an average of 71,3 (DS ± 18,8) out of the 100 possible points. Although this, mostly all the participants suffered from a chronic disease (83,6 %) and was taking an average of 2,94 pills per day (per person).
Regarding their aging, the 73,1 % declared their acceptation on the aging issue, while the 26.9 % felt fear, laziness or concern towards this process.
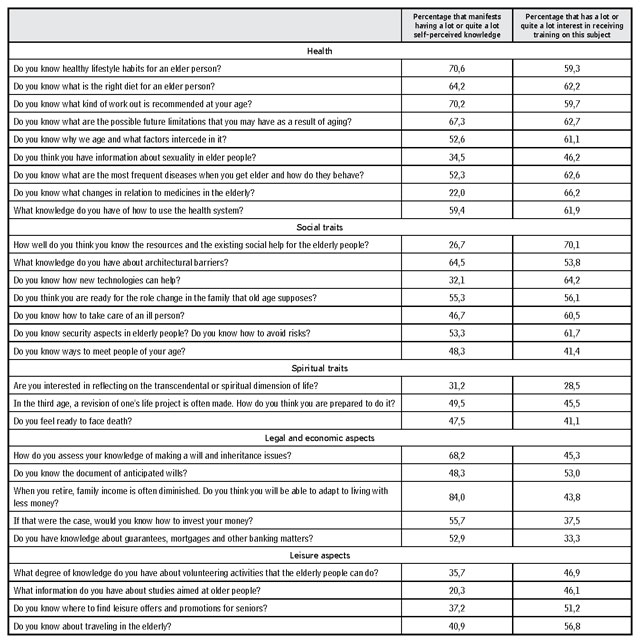
Table 1 shows the percentage of high self-perceived knowledge and of formative interest of the participants with respect to the different issues raised before, understanding as a high degree of knowledge or of formative interest when the subject answered “a lot” or “quite a lot” in the different items.
Table 1. Percentage of high degree of auto-perceived knowledge and educational interests of participants (n = 306) in Mataró (Barcelona) Spain
Source: Own elaboration.
Mainly all the participants affirmed that they had a high degree of knowledge regarding aspects related to life habits (70.6 %), an adequate diet (64.2 %), work out (70.2 %), possible future limitations (67.3 %), architectural barriers (64.5 %) and the living will (68.2 %).
However, around a 60 % of the respondents showed interest in receiving training about different aspects related to a healthy lifestyle (59,3 %), an appropriate diet (62,2 %), work out (59,7 %), possible future limitations (62,7 %), issues related to aging (61,1 %), frequent diseases in the elderly (62,6 %), taking medications (66,2 %) %), the use of the health system (61,9 %), social resources (70,1 %), new technologies (64,2 %), care of sick people (60,5 %) and security aspects (61,7 %).
Moreover, while only a 28.5 % of the subjects surveyed had completed a training course in the last five years, the 50.7 % of them said that they would take a training course on some of the previous mentioned aspects. It should be noted that the spiritual, legal, economic and leisure aspects are the least interesting among the population studied.
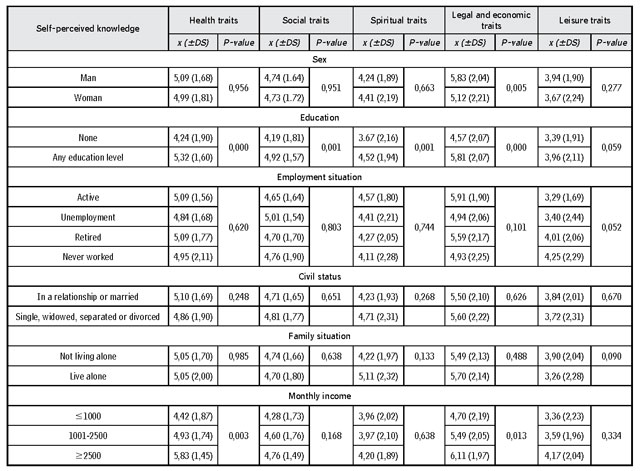
The table 2 shows the results corresponding to the relationship between the degree of self-perceived knowledge and sociodemographic aspects. It was found that a low level of education (up to primary school) is related to a lower degree of knowledge, this relationship is statistically significant (p = 0.001) in all aspects, except in leisure, where the trend is maintained in a non-significant way (p = 0,059). Likewise, in most of the aspects, men showed discreetly more knowledge, this tendency is statistically significant only in the case of the economic-legal aspects (p = 0,005). We also found an association between lower income and less knowledge, this relationship being significant in aspects of health (p = 0,003) and in economic aspects (p = 0,013). No association was found between the degree of knowledge and the employment situation, the marital status and the family situation.
Table 2. Relationship between the degree of auto-perceived knowledge and socio-demographic aspects (n = 306) in Mataró (Barcelona) Spain
Source: Own elaboration.
Finally, the table number 3 shows the relationship between training interests and socio-demographic aspects. There was a clear tendency to the greater formative interest from the women over the men in all the studied aspects, being this significant in aspects of health (p = 0,014), spiritual aspects (p = 0,021) and aspects of leisure (p = 0.038).
Table 3. Relationship between socio-demographic aspects and educational interests (n = 306) in Mataró (Barcelona) Spain

Source: Own elaboration.
Although in all aspects the highest level of studies was related to a greater educational interest, only statistical significance was found in the spiritual aspects (p = 0,040).
Discussion
The purpose of this study was to know the sociodemographic characteristics of the “young” elderly (60-70 years) of the population of Mataró (Barcelona), as well as the relationship with their knowledge and training needs perceived on aspects related to the coping of a healthy aging.
The results obtained show that there is a need for training population sector. This study has allowed to know that as people get older, they perceive that they need to know more about healthy lifestyle habits and possible future limitations in the aging process, especially on how to deal with the care of a member of the family. Yet, they would like to know and have more social and technological resources. A report from the Spanish Ministry of Health (IMSERSO, 2002) and the Health Survey of Catalonia (ESCA, 2017) already showed that, for the elder, the aspects of greatest satisfaction in their lives are their health, their fitness, their free time and their lifestyle (21,22).
The characteristics of the sample are similar to other studies which have been already carried out in the Catalan population (23). It is significant that more than half of the participants reported being in good health and that the average of those scored their self-perceived health status with 71.3 points. This shows that people perceive their state of health as good as long as it allows them to continue carrying out their daily activities autonomously (22, 24). Likewise, the results are alike to the data obtained in 2017 in the Catalonia’s population (21). It is also interesting to observe the digital literacy of the participants, who the majority of them, confirm they manage well on the internet.
Regarding self-perceived knowledge, men claimed to have more knowledge on legal and economic aspects than women. In a study that analyzed the differences between cognitive aspects and quality of life on elderly men and women, it was observed that there were differences between both genders since men had a better subjective health than women (25). However, in our study, we obtained similar results between both sexes in the rest of the scale dimensions. From another point of view, the educational level was found to be significant in all aspects of the survey: A higher level of education implies a greater degree of self-perceived knowledge. In this respect, the study by Navarro et al. (25), who found that the educational level was the major variability determinant regarding the quality of life in the elderly, beyond all the differences explained by the age or sex of the participants (25). Otherwise, it was observed that the level of monthly income was related to the health and economic-legal knowledge perceived, thus having a higher knowledge people with higher incomes. Aguilar-Palacio et al. (26) presented similar results, in which it concluded that there were differences in terms of health and the use of the health services in the elderly according to their social class. Therefore, it is necessary to ensure the accessibility and equity of health services (26).
Regarding the educational interest, women showed greater interest in all the survey aspects, a fact that can be explained by the progressive increase in the number of women living alone (27, 28). As other studies show, women have a greater need for social integration, which indicates that their interest in receiving training could be related, especially, with variables linked to the other’s support (25,28). Besides, people who were not in a relationship, or married, or who lived alone showed more interest in leisure issues. These results agree with the SOLGER study (24), which shows that people who live alone are more interested in doing social and leisure activities (24).
Literature defines in an extensive way the negative effects that can cause the role of the caregiver (29, 30, 31), although it also describes positive traits of the act of caring when the caregiver lives his task as a privilege (30). Even so, the exclusive dedication to this task makes it impossible to develop other activities that could be related to a healthy aging (32). In our population, the 28 % of them took care of a relative, and the 19 % took care of their grandchildren as their only activity. Although it is not the objective of our study, the role of the caregiver is considered relevant in relation to the possible affectation of the quality of life and predisposition to be formed of these people.
Planning aging means considering everything that can keep us active and healthy, live to the fullest and be able to meet the basic needs. In many cases, the lack of information and training can trigger situations of isolation or loss of life quality. In general, the results that emerge from this study show that older adults are interested in receiving training on different aspects of their lives to acquire knowledge that helps them maintain a good state of health during their aging. These results can help to design intervention strategies aimed at older adults to help them anticipate their needs and plan an active and healthy aging. At the same time, there is a raising in the need to have social and health resources that help older adults to occupy their free time in a satisfactory manner and without negative consequences for their own health, emphasizing facilitating the role of caregiver.
Different psychoeducational interventions directed to the caregiver have demonstrated their effectiveness in the past (30, 16, 17). An experimental study, developed by Zabalegui et al., concluded that the intervention Information, Training and Social Support (INFOSA) reduced the overload and emotional stress and improved the perceived social support of the participants (31). Similarly, other studies carried out psychoeducational interventions that showed positive effects on overload, anxiety and depression (30, 16). These studies indicate that the application of psychoeducational interventions entails significant improvements in terms of people’s health and that, in addition, the application of these interventions over prolonged periods could maintain their long-term positive effects (30, 16, 17).
Given the cross-sectional nature of the study, causal relationships between the factors studied cannot be identified. However, the results obtained allow us to better understand the degree of knowledge and the training needs perceived by the elderly in relation to how they want to face their retirement and their aging. Even so, it would be interesting to replicate the study in populations with different social classes, as well as to split the sample between retired and non-retired people in order to compare possible differences.
The nursing professional, from primary care consultations, identifies elderly people who are in a new stage of the life cycle, in which, due to ignorance or poor planning, they find themselves in situations of isolation and loneliness, which in many cases Sometimes it causes a progressive loss of health. This study will allow nursing professionals to design psychoeducational interventions adapted to the real needs of this population, which help improve their knowledge, attitudes, habits and, consequently, the health outcomes of this sector of the population.
Conclusion
The findings of this study cosign that training needs perceived by older people are fundamentally, the healthy life habits, i.e. work out and diet, the possible future limitations related to aging, the use of medicine, how the health system runs, the acces to social resources, the new technologies and, finally, their ill relatives’ care.
On the other side, it also validates that elements such as the high education level and the high social class are related to a better autopercieved knowledge of the evaluated aspects.
Moreover, it is verified a high digital literacy degree which would facilitate an educational approach though the new technologies.
After all, the conclusion is that it exists the necessity of relieving a training among the elderly population, specially women, so they can face a healthy aging. Facing this scenario, the health professionals, particularly nurses, as the closest professionals, execute a decisive role on the elderly good quality of life guarantee.
Conflict of interests: None declared.
Bibliography
1. Tyrovolas S, et al. Successful aging, dietary habits and health status of elderly individuals: A k-dimensional approach within the multinational MEDIS study. Exp Gerontol. 2014 Dec.; 60: 57-63. DOI: 10.1016/j.exger.2014.09.010
2. Organización Mundial de la Salud (OMS). Informe mundial sobre el envejecimiento y la salud [Internet]. Ginebra; 2015 [quoted 2018 May 11]. Retrieved from: http://apps.who.int/iris/bitstream/10665/186466/1/9789240694873_spa.pdf
3. Agència de salut pública. Bases per a la promoció de l’envelliment actiu i saludable [Internet]. 2014 [quoted 2018 May 11]. Retrieved from: http://salutpublica.gencat.cat/ca/publicacions_formacio_i_recerca/publicacions/actualitat/bases-per-la-promocio-de-lenvelliment-actiu-i-saludable/
4. Instituto Nacional de Estadística. Demografía y población / Padrón. Población por municipios [Internet]. 2017 [quoted 2018 May 11]. Retrieved from: http://www.ine.es/dyngs/INEbase/es/categoria.htm?c=Estadistica_P&cid=1254734710990
5. Dapp U, et al. Active health promotion in old age: methodology of a preventive intervention programme provided by an interdisciplinary health advisory team for independent older people. J Public Health. 2005 Jan.; 13(3):122-7. DOI: 10.1007/s10389-004-0097-3
6. Henning G, Lindwall M, Johansson B. Continuity in well-being in the transition to retirement. GeroPsych. 2016 Nov.; 29(4):225-237. DOI: 10.1024/1662-9647/a000155
7. Chulián A, Garrido M. Manual de preparación a la jubilación positiva. [Internet]. 1st ed. Madrid: Fundación Desarrollo y Asistencia; 2015 [Cited 2018 May 11]. Quoted from: http://www.fundacionmontemadrid.es/uploads/area/989d47ad9f1b22d990a0a84ac56793deea51850e.pdf
8. Horner E, Cullen M. The impact of retirement on health: quasi-experimental methods using administrative data. BMC Health Services Research. 2016 Feb.; 16(1). DOI: 10.1186/s12913-016-1318-5
9. Dahmen N, Cozma R. Media Takes: On Aging. Nueva York: International Longevity Center - USA; 2009.
10. Fundación Bancaria “la Caixa”. Vejez y cuidados. ¿Cómo viviremos y nos cuidaremos cuando seamos mayores? [Internet]. 2018. Retrieved from: https://observatoriosociallacaixa.org/documents/22890/121434/DOSSIER5_CAST_baixa.pdf/418e7068-e885-d6be-aa86-5beac27d7b61
11. Di Gessa G, Glaser K, Tinker A. The impact of caring for grandchildren on the health of grandparents in Europe: A lifecourse approach. Social Science & Medicine. 2016 Aug.; 152:166-175. DOI: 10.1016/j.socscimed.2016.01.041
12. Djundeva M, Dykstra P, Fokkema T. Is living alone “aging alone”? Solitary living, network types and well-being. The Journals of Gerontology: Series B. 2018 Sept. DOI: 10.1093/geronb/gby119
13. Hiel L, Beenackers M, Renders C, Robroek S, Burdorf A, Croezen S. Providing personal informal care to older European adults: should we care about the caregivers’ health? Preventive Medicine. 2015 Jan.; 70:64-68. DOI: 10.1016/j.ypmed.2014.10.028
14. Lyons J, Cauley J, Fredman L. The effect of transitions in caregiving status and intensity on perceived stress among 992 female caregivers and noncaregivers. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2015 Aug.; 70(8):1018-1023. DOI: 10.1093/gerona/glv001
15. Foster L, Walker A. Active and Successful Aging: a European policy perspective. The Gerontologist. 2014 Feb.; 55(1):83-90. DOI: 10.1093/geront/gnu028
16. Zabalegui Yárnoz A, Navarro Díez M, Cabrera Torres E, Gallart Fernández-Puebla A, Bardallo Porras D, Rodríguez Higueras E et al. Eficacia de las intervenciones dirigidas a cuidadores principales de personas dependientes mayores de 65 años. Una revisión sistemática. Revista Española de Geriatría y Gerontología. 2008 May; 43(3):157-166. DOI: 10.1016/S0211-139X(08)71176-4
17. Zabalegui A, Galisteo M, Navarro M, Cabrera E. INFOSA intervention for caregivers of the elderly, an experimental study. Geriatric Nursing. 2016 Nov.; 37(6):426-433. DOI: 10.1016/j.gerinurse.2016.06.001
18. Menichetti J, et al. Engaging older people in healthy and active lifestyles: a systematic review. Ageing and Society. 2015 Nov.; 1-25. DOI: 10.1017/S0144686X15000781
19. Institut d’estadística de Catalunya (Idescat). Projeccions de Població 2013-2051 [Internet]. 2014 [quoted 2018 May. 11]. Retrieved from: http://www.idescat.cat/cat/idescat/publicacions/cataleg/pdfdocs/pp2013-2051pr.pdf
20. National institute on aging [Internet]. USA [Cited 2018 May. 11]. Retrieved from: http://www.nia.nih.gov/
21. ESCA continue. Onada 14 (2017-1) - Qüestionari general - Població de 15 anys i més. Generalitat de Catalunya: Departament de Salut i Institut d’Estadística de Catalunya. [Quoted 2018 Jul. 17]. Retrieved from: http://salutweb.gencat.cat/ca/el_departament/estadistiques_sanitaries/enquestes/esca/resultats_enquesta_salut_catalunya/
22. IMSERSO. Envejecer en España, II Asamblea Mundial sobre el Envejecimiento. Indicadores demográficos, económicos, sociales, de salud y de servicios sociales. Madrid: Instituto de Migraciones y Servicios Sociales (IMSERSO); 2002.
23. Zabalegui A, et al. Análisis del programa educativo PECA para mejorar la calidad de vida de las personas mayores. Aten Primaria. 2006 Jun.; 37(5):260-5. DOI: 10.1157/13086310
24. Paino Pardal L, Poblet i Montells L, Ríos Álvarez L. Mayores que viven solos y malnutrición. Estudio SOLGER. Atención Primaria. 2017 Oct.; 49(8):450-458. DOI: 10.1016/j.aprim.2016.10.007
25. Navarro E, Calero M, Calero-García M. Diferencias entre hombres y mujeres mayores en funcionamiento cognitivo y calidad de vida. European Journal of Investigation in Health, Psychology and Education. 2015;4(3):267. DOI: 10.1989/ejihpe.v4i3.74
26. Aguilar-Palacio I, Carrera-Lasfuentes P, Solsona S, Sartolo M, Rabanaque M. Utilización de servicios sanitarios en ancianos (España 2006-2012): influencia del nivel de salud y de la clase social. Atención Primaria. 2016 Apr.; 48(4):235-243. DOI: 10.1016/j.aprim.2015.01.016
27. Holt-Lunstad J, Smith T, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality. Perspectives on Psychological Science. 2015 May; 10(2):227-237. DOI: 10.1177/1745691614568352
28. Gumà J, Treviño R, Cámara A. Posición en el hogar y género. Desigualdades en la calidad de vida relacionada con la salud entre la población adulta en España. Revista Internacional de Sociología. 2015 Apr.; 73(1): e003. DOI: 10.3989/2013.03.04
29. Alvira MC, et al. The association between positive-negative reactions of informal caregivers of people with dementia and health outcomes in eight European countries: a cross-sectional study. J Adv Nurs. 2015 Jun.; 71(6):1417-1434. DOI: 10.1111/jan.12528
30. Zabalegui A, Hamers J, Karlsson S, Leino-Kilpi H, Renom-Guiteras A, Saks K et al. Best practices interventions to improve quality of care of people with dementia living at home. Patient Education and Counseling. 2014 May; 95(2):175-184. DOI: 10.1016/j.pec.2014.01.009
31. Fauth EB, Gibbons A. Which behavioral and psychological symptoms of dementia are the most problematic? Variability by prevalence, intensity, distress ratings, and associations with caregiver depressive symptoms. Int. J. Geriatr. Psychiatry. 2014 Mar.; 29(3), 263-271. 10.1002/gps.4002
32. López-Casasnovas G. Una visión de futuro de las políticas de salud. Gaceta Sanitaria. 2009 Jul.; 23(5):458-461. Retrieved from: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0213-91112009000500017